Pioglitazone reduces cardiovascular events and dementia but increases bone fracture in elderly patients with type 2 diabetes mellitus: a national cohort study
“In results, the pioglitazone group (n = 17,388) exhibited a lower rate (per person-years) of major advanced cardiovascular events MACCE (2.76% vs. 3.03%, hazard ratio [HR]: 0.91, 95% confidence interval [CI]: 0.87–0.95), new- diagnosis dementia (1.32% vs. 1.46%, HR: 0.91, 95% CI: 0.84–0.98) but a higher rate of new-diagnosis bone fractures (5.37% vs. 4.47%, HR: 1.24, 95% CI: 1.19–1.28) than the non-pioglitazone group (n = 174,549). In conclusion, using pioglitazone may reduce the risks of MACCE and dementia but increases the probability of bone fractures in the elderly DM population.”
This study was mentioned further up in this thread:
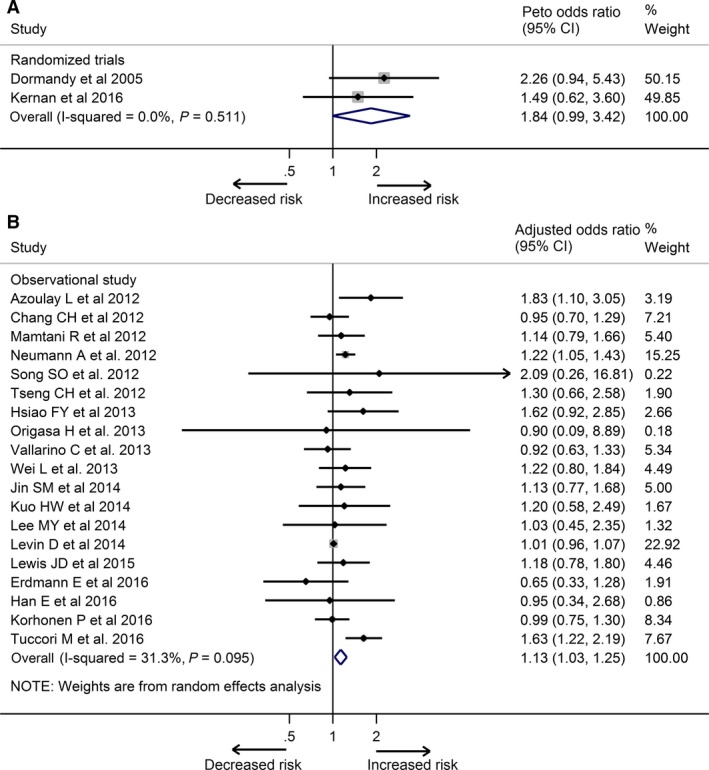
Pioglitazone use increases risk of Alzheimer’s disease in patients with type 2 diabetes receiving insulin
Note, these are insulin dependent diabetics.
What if insulin was removed from the equation:
Effect of pioglitazone medication on the incidence of dementia
"Long-term use of pioglitazone was associated with a lower dementia incidence. Relative to nondiabetics, the cumulative long-term use of pioglitazone reduced the dementia risk by 47% (RR = 0.53, p = 0.029). If diabetes patients used pioglitazone <8 quarters, the dementia risk was comparable to those of nondiabetics (RR = 1.16, p = 0.317), and diabetes patients without a pioglitazone treatment had a 23% increase in dementia risk (RR = 1.23, p < 0.001). We did not find evidence for age effects, nor for selection into pioglitazone treatment due to obesity.
Interpretation: These findings indicate that pioglitazone treatment is associated with a reduced dementia risk in initially non-insulin-dependent diabetes mellitus patients. Prospective clinical trials are needed to evaluate a possible neuroprotective effect in these patients in an ageing population."
Lower risk of dementia with pioglitazone, compared with other second-line treatments, in metformin-based dual therapy: a population-based longitudinal study
Effects of pioglitazone on the incidence of dementia in patients with diabetes
“Pioglitazone is a time- and dose-dependent protective factor against dementia in patients with diabetes. The risk of dementia is lower in long-term and high-dose pioglitazone users than in never users of pioglitazone.”
Pioglitazone Use and Reduced Risk of Dementia in Patients With Diabetes Mellitus With a History of Ischemic Stroke
“Pioglitazone use was associated with a reduced risk of dementia, compared with nonuse (adjusted hazard ratio [aHR] = 0.84, 95% CI 0.75–0.95); the risk reduction in dementia was greater among patients with a history of ischemic heart disease or stroke before DM onset (aHR = 0.46, 95% CI 0.24–0.90; aHR = 0.57, 95% CI 0.38–0.86, respectively). The incidence of stroke was also reduced by pioglitazone use (aHR = 0.81, 95% CI 0.66–1.00). However, when the stroke developed during the observation period of pioglitazone use, such lowered risk of dementia was not observed (aHR = 1.27, 95% CI 0.80–2.04).”
Ralph DeFronzo Banting Hall lecture from some years ago, getting into the details of insulin resistance in the context of atherosclerosis. There is a lot of cellular and molecular information which I think gives us a good picture of the processes involved. There is also light thrown on pioglitazone, as he says “the only true insulin sensitizer”:
Banting Hall - Dr. Ralph A. DeFronzo (via Diavcon 2020)