Then again, do more males develop diabetes on statins than women or is it the opposite?
Similarly, the cancer point that was raised above (though in older patients), to the extent that is mediated via impairments in metabolic health/glucose control from stations, might be a larger risk for men than women.
Deaths from cancer were statistically significantly lower in the statin group though.
Neo
#84
These are exactly the type of questions we have to ask.
We have to go beyond the averages in the trials and do everything we can to integrate all relevant info and triangulate things to the individual person. Age, gender effects? Differences in a person at risks of metabolic syndrome vs someone that has other risks. Is the person a cholesterol over absorber or over provider.
What is the response to a given medicine when trialed? Do you stick, change the mix or put on the shelf and try something else.
1 Like
Or just add more pills to the mix. Rosuva/Atorvastatin, ezetimibe and acarbose make for a great combination.
1 Like
Neo
#86
From this one study that does not seem to be the case for the older group. Or what am I missing:
Results
We included 27 trials with 188’259 participants (23 statin; 4 ezetimibe trials). The trials reported 4056 cancer deaths, 2061 under LLT and 1995 in control groups. Overall, there was no increased risk of cancer mortality (RR 1.03, 95% confidence interval 0.97–1.10), with no difference between primary and secondary prevention. In the subgroup analyses for RCTs with ≥15% of participants aged ≥75 years, the RR of cancer death was 1.11 (1.00–1.23), while the RR for CV death was 0.96 (0.91–1.01). For RCTs with a mean age ≥ 70 years, the RR for cancer death was 1.21 (0.99–1.47).
Conclusion
LLT does not lead to a shift from CV to cancer death. However, there might be a possible shift with a pattern of increased cancer deaths in trials with more older adults, particularly ≥75 years. Individual participant data from LLT trials should be made public to allow further investigations.
—-
Above is just one paper that someone referred too and I’m haven’t look what the overal literature suggests
I didn’t not mean to empathize this one question
I was more trying to say how personalized medicine is possible beyond just looking at the headline levels of RCT and going blindly with that without integrating all of types of info that can help guide the tradeoff decisions one has to make.
1 Like
adssx
#87
I think low-dose combinations are the way to probably get most benefits while minimizing adverse effects. Or is it wishful thinking? (I want to see rosuvastatin 2.5 mg + ezetimibe 5 mg + bempedoic acid 90 mg, or even lower doses, I asked George Medicines if it was in their plans…)
Definitely. Like if you have a history of UTI and genital infections, don’t get SGLT2 inhibitors no matter how good they can be. If your diabetes is not well controlled fixed that first and/or prefer BA/EZE to statins. But we also want to know if there’s a clear “general” winner in a category for people who are “healthy” without falling in a specific common group.
2 Likes
A_User
#88
How much can we trust a meta analysis? It was also a mix of all the statins and ezetimibe. Look at the forest plots, all statistically insignificant. Do you have a study on statins on ACM in above 75 yrs old?
How do you know your approach is better?
Neo
#89
Re first one as I mentioned
Re the second one:
I’m not saying any info is additive, but I am saying that key important data is, like ALSO looking at MRs, ALSO taking into account meta analyses, and/or ALSO taking into the massive amounts of mechanistic understanding in this type of area where the body of fundamental understanding is large. If you think MR only should have X% of the weight of RCTs, then you just give it that weight in your decision making framework, but it will likely not be 0% for the best possible ex ante expected decision making quality.
Other arguments are listed above - feel free to raise concerns about the specific arguments (e.g. taking into account over absorber vs over producer of cholesterol, taking into account how you feel and what changed is your broader blood work when fir trialing a cholesterol modulating medicine, etc).
Another framework, that roughly captures the issue from my view, is that you are talking about things above in a Medicine 2.0 way when you are smart and well read enough that you can begin applying Medicine 3.0:
See for instance The evolution of medicine and the transition to “Medicine 3.0” from round 3min to 11min 45sec in link below
(Better covered in his book if I recall correctly)
2 Likes
A_User
#90
I think you are missing my point. You might reduce LDL and apoB more in one strategy over the other, however if there is no signal of net benefit, meaning in all cause mortality, it is a proven inferior strategy.
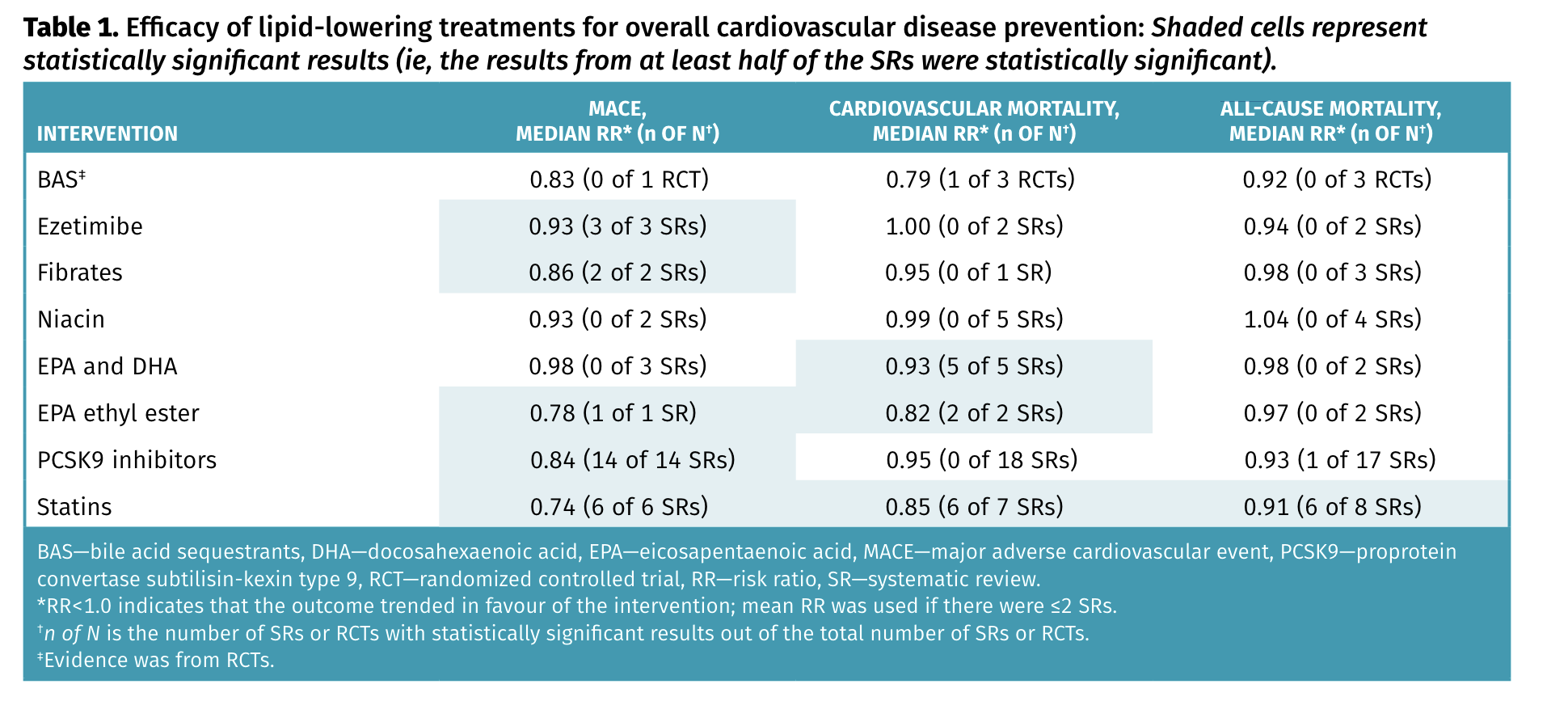
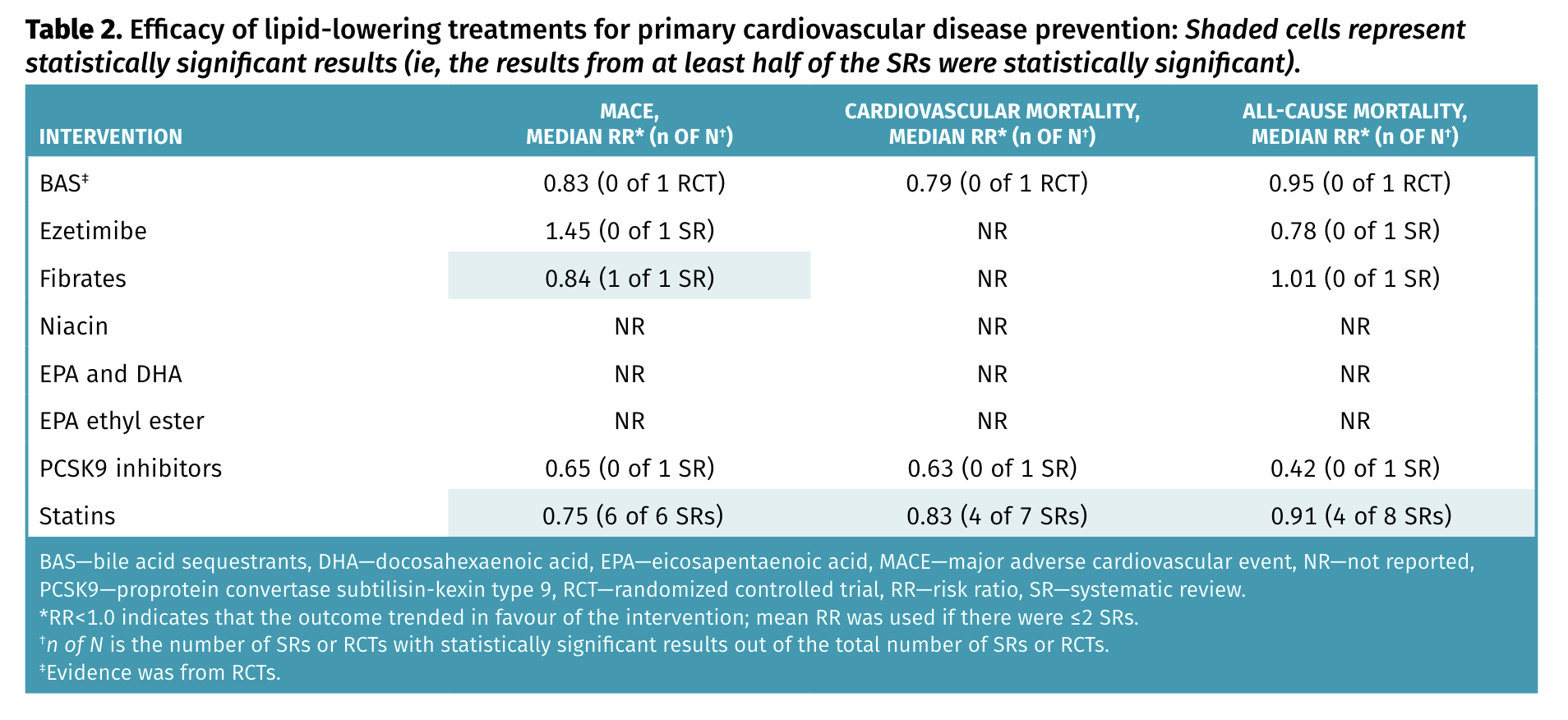
See the tables posted by adssx:
Statins have detected a decrease in all cause mortality in most systematic reviews, the same for cardiovascular mortality, both for primary and secondary prevention. PCSK9i have ACM decrease detected in one review for secondary prevention.
You might increase your mortality with PCSK9 inhibitors, while certainly not for statins. So you can be in zone of “not knowing”, “unknown”, or be in the zone of knowing/known, take statins, and wait for more data.
Neo
#91
I feel it is the other way around.
Neither of those two tables apply in a good, straight 1-to-1 mapping way to my understanding of you or me - we would not have met the criteria to enroll in those trials (and almost none of those patients were in their 20s which I believe you are?, those data are for an average of male and female and I guess you only have one biological sex, etc) and hence the average from those trials does not apply to you in a black and white and perhaps not even in a great/good way.
And as long as that data is imperfect you can do better by also (as in “and” and not “instead”) looking at other good knowledge to cross triangulate. Are you saying that all other possible other data has zero value if combined with the type of data in the table?
Don’t want to spend more time on this. If you still feel we are far apart, we can agree that you feel I’m missing your points and I feel that you are missing my points and leave it as that.
1 Like
L_H
#92
I’m curious what you think of a rotation strategy for apob lowering drugs. I appreciate there’s no evidence to support it, and that there’s a risk you might have sides from a specific drug. But given the length of time you’d be looking to take these, would rotating between statins, ezetimibe, psk9i and bempedoic a (and combinations thereof) be a sensible precaution?
I guess the logic would be that very long term use could lead to an accumulation of sub-clinical (silent) but longevity-impairing side effects. I’m thinking there are likely to be a multitude of subtle impacts that we don’t know about yet. And some things we do know about. So we might avoid prolonged higher uric acid by rotating bempedoic a, and avoid prolonged lower omega 3 by rotating out ezetimibe etc etc.
But mostly it would be insurance against putting all your longevity eggs in one pharmaceutical basket.
2 Likes
I guess not before 2026.
Yes, sure, but this is all based on RCTs that have average length of what? 4 years?
Yes, I like this approach too. Lowest affective dose and multiple pathways.
This approach also seems reasonable. However, how would you organize your treatment cycles? It seems logical to alternate between drugs every few months, but taking full doses and relying on a single pathway may not be as effective. Perhaps shorter cycles could be considered. For example, in lipid-lowering therapy, one could use a weekly statin combined with low-dose ezetimibe EOD or E3D. Studies have shown effectiveness with this approach and pathways are not blocked continuously. It’s possible that BA could also demonstrate some effectiveness in such an intermittent schedule. Further research and clinical trials would be needed to explore its potential in this context.
1 Like
A_User
#94
That data is much better than a similar and even more imperfect data (no detection of ACM). The discussion is about one drug relative to another and which is better.
Like I said to @Neo it is a discussion about one drug relative to another.
adssx
#95
Two Dutch researchers commented on the CLEAR Outcomes trial results:
Evaluating the effect of bempedoic acid on kidney function: call for cautious implementation 2024
Ray and colleagues reported an increased incidence of kidney impairment under bempedoic acid compared with placebo in their appendix, particularly in patients with prediabetes or diabetes, which appeared to be largely attributable to elevations in creatinine concentrations from baseline. This finding is similar to previous research indicating a reversible 6% increase in creatinine concentrations with bempedoic acid treatment.
Yet, the authors also noted persistent increases in blood urea nitrogen with bempedoic acid, which could indicate genuine kidney function decline besides isolated transporter effects. Furthermore, the increased incidence of muscle-related adverse events (odds ratio 0·75, 95% CI 0·55–0·99; p=0·046) together with a baseline weight-adjusted mean weight loss of 0·64 kg could have indicated potential treatment-related muscle loss.
The original authors answered: Evaluating the effect of bempedoic acid on kidney function: call for cautious implementation – Authors’ reply
The numerically increased rates of adverse events summarised under the heading renal impairment reflect small changes in renal laboratories (eg, increased creatinine, decreased eGFR, or increased BUN) rather than clinically meaningful acute or chronic changes in renal function. Acute kidney injury occurred in 1·1% of patients receiving bempedoic acid and 1·0% of patients receiving placebo, and renal failure occurred in 1·1% of patients receiving bempedoic acid and 0·9% of patients receiving placebo; 0·2% of patients in both treatment groups had an eGFR less than 15 mL/min per 1·73m2 at any time during the trial.
Thus, the comprehensive clinical data suggest that the small changes in creatinine and BUN do not appear to be of clinical significance and are independent of the small changes in weight seen in people with obesity.
4 Likes