First question which I didn’t see anywhere: how old are you? From other comments, I’m guessing 50?
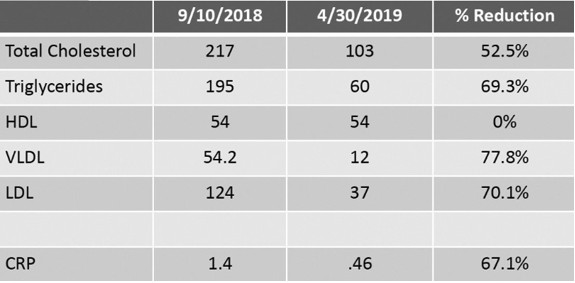
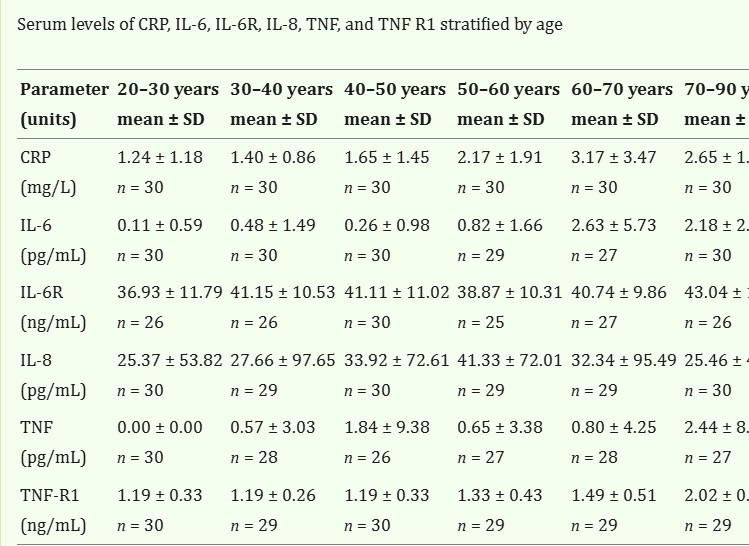
CRP of 1.67 isn’t really that high IMO. I’m not expert in this, but I seem to observe that some people have very different baselines. 1.67 vs 1.59 almost certainly does not represent any sort of change.
Total testosterone is great IMO. The lab is using some weird cutoff where 700-1000 is normal. In reality, that’s like the upper 20th percentile. (doi:10.1371/journal.pone.0109346). 579 is a perfectly normal number.
The free testosterone is definitely more mysterious. What time of day was the blood test? (Again, SHBG is totally fine, and not actually low).
MCV of 93 is totally normal. Saying 84-91 is “optimal” is not supported by evidence that I know of.
I also wouldn’t worry about IGF-1. This number alone doesn’t mean much. And after all, IGF-1 plays very useful roles, and I would never stop taking protein supplements because of a serum IGF-1 blood test.
Monocytes and lymphocytes are totally fine. And anyway, these are % numbers. What matters more is the actual concentration of cells.
ALT and AST are both high. But GGT is low. So to my eyes, that means your liver is probably fine, and these are being released from somewhere else - probably muscle.
I agree with others that you might have had some infection which you didn’t consciously register. That could explain almost everything, including the raised fibrinogen.
Also, I gather you’re from HK, but on holiday in the USA… did you think of the massive disruption to your circadian rhythm? Testosterone, IGF-1 etc all normally follow a circadian rhythm, and you’ve just switched time zones by 10-12 hours.