Well, most seems at the 300 mg/kg dose and drops off at 700 and higher (1000). But note early termination, not favorable trends. Dose, poison etc. Some sex differences.
adssx
#1605
Amazing, thanks for sharing. So dapagliflozin and empagliflozin also increase lifespan in male mice. (We already had one Chinese paper on empagliflozin confirming that.) So it’s not only an SGLT1 effect @Neo.
Using the FDA conversion guide, 100 mg/kg = 650 mg/day, in a 80 kg human. The maximum approved dose is 25 mg/day. So there is no risk. But do empa and dapa also increase lifespan at these low doses?
7 Likes
adssx
#1606
Dapagliflozin alleviates mitochondrial damage in the myocardium under diabetic conditions by targeting sortilin 2025
Our findings uncover a novel molecular mechanism through which dapagliflozin improves myocardial mitochondrial injury under diabetic conditions, suggesting SORT1 as a potential therapeutic target for treating myocardial injury in diabetes.
3 Likes
Neo
#1607
Can you talk more to this?
1 Like
Neo
#1608
Will take a look.
@A_User @adssx - Is this a 2013 packet? But the result was never published in a paper?
2 Likes
A_User
#1609
That’s from the 104 week (2-year) carcinogenicity rat or mouse study that it seems most drugs have to do.
See this post:
3 Likes
Jay
#1610
blsm, I think of exercise as being 4 to 5 zones with a level 2 being a steady walk (and talk) for a mile or two before moving into a fast walk with very limited conversation as zone 3. From there it’s jogging (level 3) and sprinting (level 4). Can you describe your zone 2? I ask because I’ll be trying Empagliflozin soon, but I hate to think that it could mess up my exercise routines.
1 Like
Neo
#1611
@A_User @adssx
Did you see Matt K’s comment on the other thread:
”(2) Lifespan studies are not carcinogenicity studies. Perhaps that wasn’t what the comment intended, but this is what it sounded like.”
What are your thoughts? I’d rather believe your point that this FDA packet provided longevity data - but is Matt saying that it is not that helpful? Or did he not understand the packet?
1 Like
A_User
#1612
I think Matt was addressing a separate point as
“… at relativley low cost (compared to the cost of moving an unworthy drug forward) in less than a year by starting in 24 month old mice.” and
“… assuming the goal is a geroprotector, not an incremental disease drug.”, etc, sound to me that Matt believes they were carcinogenicity studies in name only, basically what those studies are called.
The everolimus study I posted in that thread seems to have had a nice +25% effect on 104 week lifespan compared with control, and decrease in age-related effects, statistical significance testing aside, if you can take a look and if you agree.
2 Likes
blsm
#1613
Sure, I can’t decide if this change is good or bad yet. At first I was leaning towards good but now I’m not so sure. Here’s a little background and caveats: I’m a 55 y/o female, not an athlete or very knowledgeable about fitness but I’m pretty active. Fitbit fwiw gives me an excellent cardio fitness score of 43-47.
I average 10k steps per day, do sprint intervals for 15 minutes 1x/week, ruck for @40 minutes with 10-25% of my body weight 4-5x/week and lift weights 2-3x/week. I could easily achieve my goal of 40 total zone minutes per day without having to try before starting dapagliflozin. Fitbit breaks them down into moderate, vigorous and peak and around 75-80% of my zone minutes would be moderate and the remaining 20-25% vigorous/peak. I also wear a 10% weighted vest around doing my normal daily activities for a minimum of 2-4 hours daily but sometimes more.
I used to at least be in zone 2 or moderate for most of the time anytime I rucked and now doing the same thing I may not get my heart rate above 100 at all or for less than 5 minutes. I ruck on uneven terrain with small hills. I did discover recently that I can get into zone 3 or higher fairly easily on a stationary bike at the gym so perhaps it’s coincidental that I noticed this shortly after starting dapagliflozin and I’m simply adapted to rucking and needed a new challenge?!?!
It seems to be doing something good for my cardiovascular system so far where I have to work harder than I used to get into zone 2 or higher but perhaps I’m interpreting things incorrectly? I’m considering getting a more detailed tracker and I’m trying to learn and understand all of this more. I didn’t really start working on my fitness until 5 years ago and didn’t really need to understand it much to see results until recently. My husband says I’ve plateaued. I hope that long winded rambling helps!
3 Likes
59vw
#1614
@blsm
Fitbit fwiw gives me an excellent cardio fitness score of 43-47.
I average 10k steps per day, do sprint intervals for 15 minutes 1x/week, ruck for @40 minutes with 10-25% of my body weight 4-5x/week and lift weights 2-3x/week.
Just had to comment… pretty impressive! Finding the time to do all that is part of the difficulty. I do a walk the dog ruck that helps kill two birds.
I think the Attia/Inigo San millan crowd defines exercise routines into three zones. Zone 1 is (I believe) similar metabolically to zone 2 but not maxing out the pathway. Zone 2 is defined as the point where you are maximizing your mitochondrial respiration for the production of ATP and generally corresponds to somewhere around 80% of maximal heart rate. Thus you are burning fats and getting maximal ATP from the process and not producing a lot of lactic acid. As you hit the next zone 3 you are unable to keep up with the activity using respiration so you begin using less efficient but more readily available energy substrates that are converted to ATP by anaerobic pathways and you begin to accumulate lactic acid.
2 Likes
blsm
#1615
Thank you! I’m trying to understand all of the better! @Joseph_Lavelle has been very helpful as well! I love this place.
1 Like
adssx
#1616
Effects of Empagliflozin on Sarcopenia Risk, Body Composition, and Muscle Strength in Type 2 Diabetes: A 24-Week Real-World Observational Study 2025
Turkish paper + MDPI so low quality but:
Results: The empagliflozin group showed significant improvements in HbA1c, fasting plasma glucose, body weight, waist circumference, and fat mass (p < 0.05 for all). No significant changes were observed in the empagliflozin group after 6 months in appendicular skeletal muscle mass index (from 7.81 ± 1.33 kg/m2 to 7.84 ± 1.38 kg/m2, p = 0.154). No statistically significant changes were observed in handgrip strength in either group.
Conclusions: Empagliflozin treatment over six months led to favorable changes in metabolic parameters and fat mass without detrimental effects on skeletal muscle mass or muscle strength. In clinical practice, the selection of antidiabetic therapies should consider individual glycemic targets, cardiovascular and renal risks, weight management, comorbidities and sarcopenia risk. Resistance exercises and adequate dietary protein intake should be recommended to preserve muscle mass in at-risk patients. Larger randomized trials are needed to confirm the long-term effects of SGLT2 inhibitors on body composition particularly in older adults.
11 Likes
adssx
#1617
Sodium-glucose cotransporter-1 inhibition and depression: A Mendelian randomization study 2025
Results: Our results indicated that genetically predicted sodium-glucose cotransporter-1 inhibition was negatively related with depression risk (ORIVW = 0.78; 95% CI: 0.67–0.91, p = 0.002) in the European population. However, we did not find a causal association between sodium-glucose cotransporter-2 inhibition and depression (OR IVW = 0.98; 95% CI: 0.71–1.36, p = 0.919).
5 Likes
Just spit balling but this points to gut health as a possible mechanism here, given SGLT1-inhibition occurs in the GI. I wonder if there have been any studies looking at SGLT1-inhibitors and gut health specifically.
1 Like
blsm
#1619
Personal anecdote:
I’ve been on dapagliflozin a little over a month and I’ve worked up to taking 5mg from 2.5 initially. I’m now able to tolerate restaurant meals without any fluid gain. I still try to make the best choices (lowest sodium) possible when eating out and stick with a no added salt diet otherwise but it’s a very welcome change to not deal with 2-3 pounds of fluid that would stick around for several days. I had gotten to the point of dreading dining out which was a shame because it’s a somewhat regular social activity amongst my family and friends. I do not have diagnosed cardiovascular or renal disease and I’m not diabetic but this medication has turned out to actually be my favorite longevity intervention. Obviously something wasn’t working optimally in my body. I also no longer have sock marks when I take my socks off which is pretty neat. My BP and weight haven’t changed and both were already optimal so I’m happy.
10 Likes
adssx
#1620
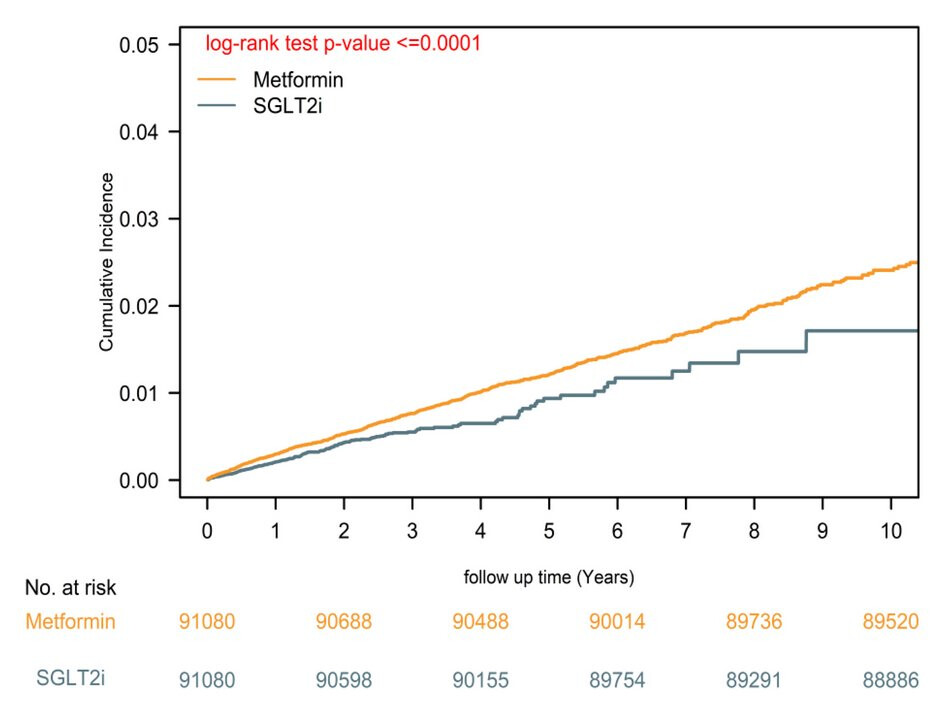
SGLT2 inhibitors vs. metformin for Parkinson’s disease risk reduction in type 2 diabetes 2025
SGLT2i use was associated with a 28% lower PD risk than metformin (aHR = 0.72; 95% CI, 0.62–0.84; p < 0.0001). Dementia, a positive control, also showed reduced risk (aHR = 0.73; 95% CI, 0.68–0.78; p < 0.0001), reinforcing the neuroprotective effect. Negative controls confirmed specificity. SGLT2i users had significantly lower all-cause mortality (aHR = 0.85; 95% CI, 0.83–0.89; p < 0.0001).
10 Likes
Nice study, thanks. The ACM benefit was small, but good to see it, 15%.
In the forest plot of figure 2, we can see that these were beneficial in statin users. And the confidence intervals were good. Does that tell us anything about statins and PD?
Do we know which specific SGLT2i are commonly used in China, or in this particular setting? I’m wondering if this is a broad class effect or there is some particular drug that predominates here.
1 Like
adssx
#1622
I don’t think we can conclude anything from that.
1 Like
adssx
#1623
It seems that dapagliflozin has the vast majority of the Chinese market: 2024年七大类降糖药解析:SGLT2i为何成指南首选?_摩熵医药(原药融云)
3 Likes