Alex2
#267
I stared taking empagliflozin 10mg. Felt hungry on it at the end of the day - I guess my body guessed there was less calories in me compared to what I ate. Unfortunately I got a fungal infection - an unpleasant but known side effect. I spoke to one of the drug reps for the company and they reassured me this usually a one off thing but hey their job is to sell the product. I think I will have to stop - I think this will happen again as I am on Rapamycin. I may take it if I know I will be eating lots of carbs like pasta but but diet is fairly low carb ( not keto ). I already take metformin long acting so I’m not sure this is for me.
Not sure if others are thinking of sglt2 inhibitors but just letting everyone know there are side effects with these drugs.
2 Likes
scta123
#268
Too bad. I have Empagligozin at home since few months and wanting to try it but was afraid of getting bacterial or fungal infection. Now I am even more reluctant to try.
Hope you are ok now and that it wasn’t too unpleasant.
bizgoz
#269
I just want to add to this. I’ve been taking Cana as a longevity agent for about 2 years. Only side effect I’ve had (and continue to have) is if I eat alot of carby foods, my urine smells “sweet”, which is not really a surprise. It also lowered my nighttime glucose level, which for unknown reasons would spike in the middle of the night during sleep before coming down to normal by the AM. (I used a CGM or never would have known this.) I’m not and never was insulin insensitive. Since Cana, I don’t get those nighttime peaks anymore. I’ve gone through a couple of periods where I experienced fatigue, but I can’t attribute it to the Cana; it could have been anything. Both times resolved itself after a couple of months and I haven’t felt that fatigue in several months.
I orignially started with 100mg, 1x day, now I break the 300’s in half and take half (150mg) once each day. When I first started it, I lost about 7 pounds over the ensuing early weeks, now I eat whatever I want and my weight remains consistent, regardless of what I eat or how much I exercise (or not).
From where I sit, the data continues to be encouraging and I have no plans to switch to Empa or anything else…
5 Likes
rapdog
#270
Does anyone know if it’s safe to split the 25mg Empagliflozin for a half dose? Thanks!
It seems that Yes…
EMP-25 tablet is relatively a flat elongated tablet making splitting easier . Using preferably a pill-cutter, the patients were shown how to cut the EMPA-25 tablet into two halves
Source: Treatment Outcomes of Graded Dose of Empagliflozin in Type-2 Diabetes: A Real World Study - PMC
More:
- Empagliflozin 25mg tablets. Dispense 45 to last 90d. Take ½ = 12.5mg daily to prevent complications of type 2 diabetes.
3 Likes
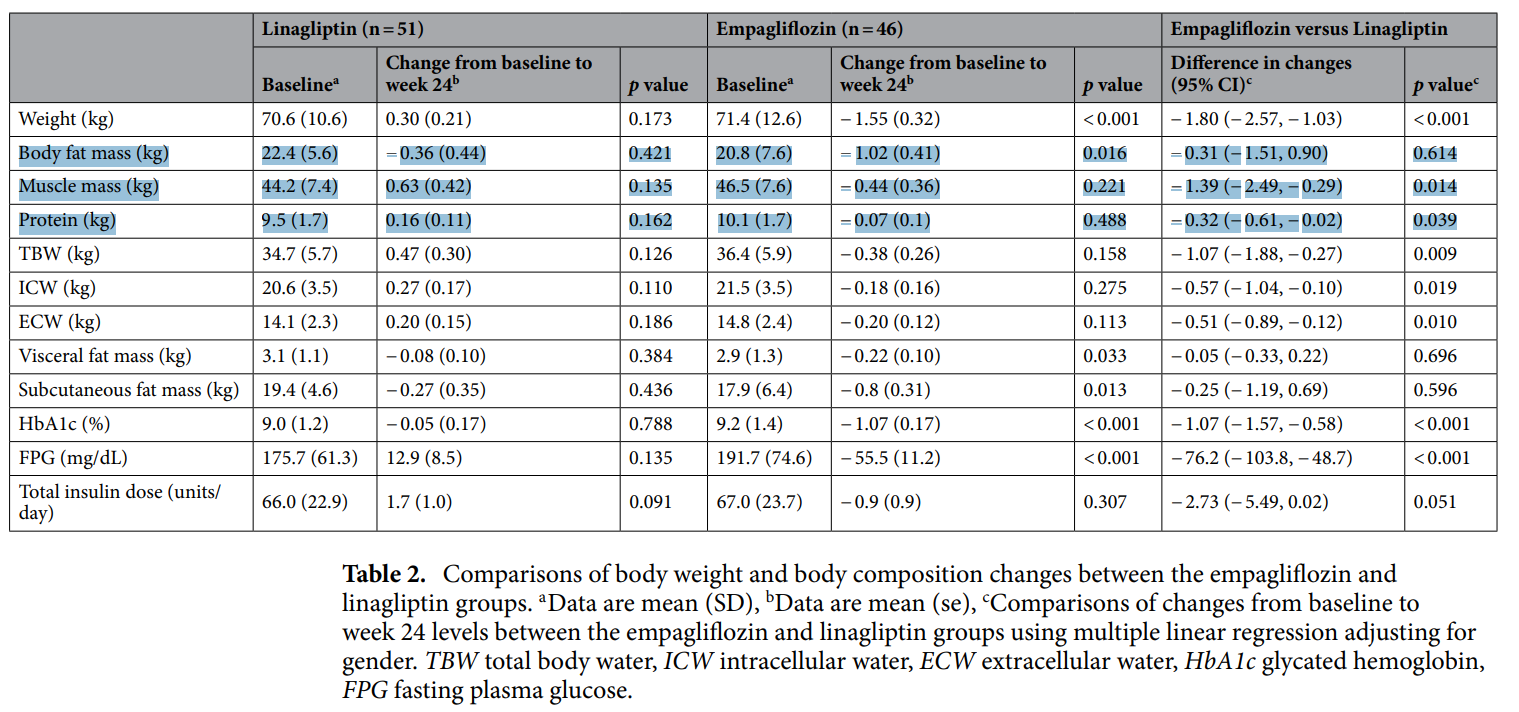
- Empagliflozin vs Linagliptin
- I switched from empagliflozin about 3 months ago because I was concerned that empagliflozin might be hindering or even lowering muscle mass gains.
- Since metformin is known to retard muscle mass increases from resistance training, I didn’t need two things slowing the results from resistance training.
- The main difference I have found is that linagliptin does not lower fasting glucose as much as empagliflozin.
FWIW: Linagliptin is about half the price of empagliflozin.
Just something to consider, I am not recommending anything.
- Empagliflozin
- Provides better glycemic control than linagliptin
- Decreases more muscle mass and total body water than linagliptin
- Provides clinically relevant placebo-corrected reductions in HbA1c
- Linagliptin
- Improves insulin secretion
- Reduces glucagon production
- Slows gastric emptying
- Promotes satiety
- Reduces appetite
- Lacks severe hypoglycemia
- Weight neutral
- Well tolerated
- Slows down renal progression
- Improves renal disease
Empagliflozin And Linagliptin (Oral Route) Description and Brand Names - Mayo Clinic.
https://www.nature.com/articles/s41598-022-21486-9
2 Likes
Hi!
Curretly taking Jardiance 25mg, I started it something like 2 years ago. Great med. You pee a little bit more but my blood sugar is way more stable (checked by FreeStyle 2). I’m in France, and it’s only 38€ a month (something like 45 dollars), and 100% payed by the social care service.
I really enjoyed this médication, hope it will protect my heart and kidneys
3 Likes
scta123
#275
Do you have T2D or are you taking it just for longevity?
I’m taking it for longevity and health purpose only. I’m 21!
3 Likes
rapdog
#277
I really appreciate your thorough and well-researched responses.
3 Likes
Neo
#278
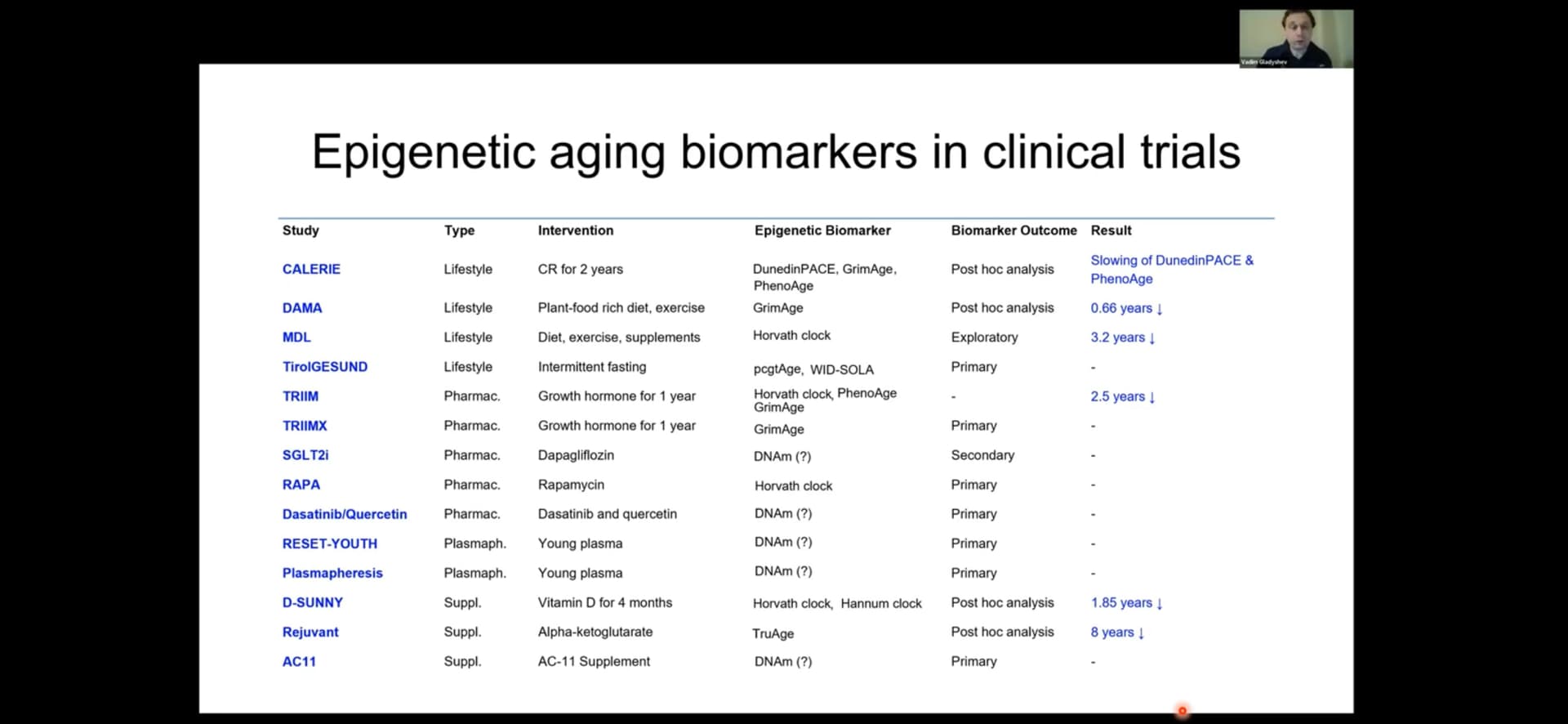
I saw below in a talk given by Harvard’s Prof Vadim Gladyshev
Does any know what the SGLT2i aging clinical trial where they are measuring epigentic age is? The seventh from the top.
(How about the rapa trial, the eighth from the top)
From here (you may enjoy the overall talk)
3 Likes
“Sotogliflozin (Inpefa) in addition to SGLT2 blockade it also blocks SGLT1, which is primarily located in the intestinal wall.“
Anyone know anything about this Sglt2 inhibitor?
Neo
#280
No. But I think Cana that was used in the ITP with success also has some SGLT1-inhibition and that the other ones generally do not do SGLT1-i, but only SGLT2-i.
1 Like
Its not available in India yet. And strangely it was withdrawn from the EU this year, the same year it was approved in the US…
This is really strange… why would you go through all the expense and effort to get a drug approved and then withdraw it two years later. Anyone find any info on the reason for the withdrawl?
public-statement-zynquista-withdrawal-marketing-authorisation-european-union_en.pdf (97.8 KB)
1 Like
Ah - found it… I think the danger is likely exaggerated (in the publication cited below), but good to be aware of it…
Before the FDA issued its decision on whether or not to approve the drug, the FDA’s Endocrinologic and Metabolic Drugs Advisory Committee reviewed the clinical trial data. The committee voted on whether or not it recommends that the FDA approve the drug. While the FDA is not required to follow the committee’s advice, it typically does. The committee was split on Zynquista. Eight members voted for approval of the drug, and eight voted against. Those that voted against were particularly concerned about the risk of diabetic ketoacidosis.
“I think it’s impossible to understate the concern about DKA (diabetic ketoacidosis) really just because the absolute increase is really remarkable,” Michael Blaha, MD, of Johns Hopkins Ciccarone Center for the Prevention of Heart Disease in Baltimore told MedPage Today at the time. “I am concerned about the prospect that this could be worse in the real world [outside of the trial setting].”
In March of 2019, the FDA officially rejected the approval of Zynquista (sotagliflozin). Lexicon and Sanofi ended their collaboration, and only Lexicon kept working on the drug. The company appealed the FDA’s decision, but the FDA stood firm and rejected that appeal in December of 2019. Meanwhile, the European Medicines Agency (EMA)—the European Union’s FDA equivalent—decides to approve the drug as an add-on to insulin treatment for those with Type 1 diabetes in April 2019.
3 Likes
Comparison of canagliflozen to Sotagliflozin. A mixed bag but I’d say Cana is a fine drug for glucose control even if sotaog has a longer lasting effect.
1 Like
I agree.
Overall, this study suggests about 11% of users discontinued using SGLT2 inhibitors due to side effects (which I don’t consider too bad… about 90% continued ).
Side effects perceived to be related to adjuvant therapy
Side effects perceived to be related to the therapy were more commonly reported by GLP-1RA versus SGLT2i users (63.2% versus 36.6%, respectively). Gastrointestinal symptoms were the most reported side effects among GLP-1RA users (57.4% versus 1.2% of SGLT2i users; Figure 1(c)). Overall, among SGLT2i users, 11.8% reported genital mycotic infections, 9.0% reported urinary tract infections (UTIs), and 11% reported polyuria/dehydration. DKA was reported by 4.9% SGLT2i users and no GLP-1RA user. No episodes of pancreatitis were reported. Of the 43 GLP-1RA users who reported side effects, less than a third (32.3%) discontinued therapy because of the side effects (22.6% of all GLP-1RA users). For SGLT2i users, 9/30 patients (30%) who experienced side effects discontinued because of the reported side effects (11% of all SGLT2i users). Among those treated with SGLT2i in Poland versus United States, the nature and frequency of the reported side effects were comparable.
Source: Patient-perceived benefits and risks of off-label use of SGLT2 inhibitors and GLP-1 receptor agonists in type 1 diabetes: a structured qualitative assessment - PMC
2 Likes
Neo
#286
Just discussed this earlier today:
Seems like this could be addressed / monitored via continuous ketone monitoring (CKM)?
2 Likes