More good news on SGLT2 inhibitors:
Highlights
• Henagliflozin can extend telomere length
• Henagliflozin affects the insulin-like growth factor-1 system and immune cell function
• Henagliflozin can lead to changes in various metabolites
• This clinical trial demonstrates the anti-aging potential of SGLT2i
Full Paper (open access)
Effect of henagliflozin on aging biomarkers in patients with type 2 diabetes: A multicenter, randomized, double-blind, placebo-controlled study
https://www.cell.com/cell-reports-medicine/fulltext/S2666-3791(25)00404-5
AI Summary:
Here’s a detailed summary of the attached Cell Reports Medicine paper:
Citation
Zhang et al. (2025). Effect of henagliflozin on aging biomarkers in patients with type 2 diabetes: A multicenter, randomized, double-blind, placebo-controlled study. Cell Reports Medicine, 6:102331. https://doi.org/10.1016/j.xcrm.2025.102331
Background
- Type 2 diabetes mellitus (T2DM) is closely tied to accelerated aging, driven in part by cellular senescence and chronic inflammation.
-
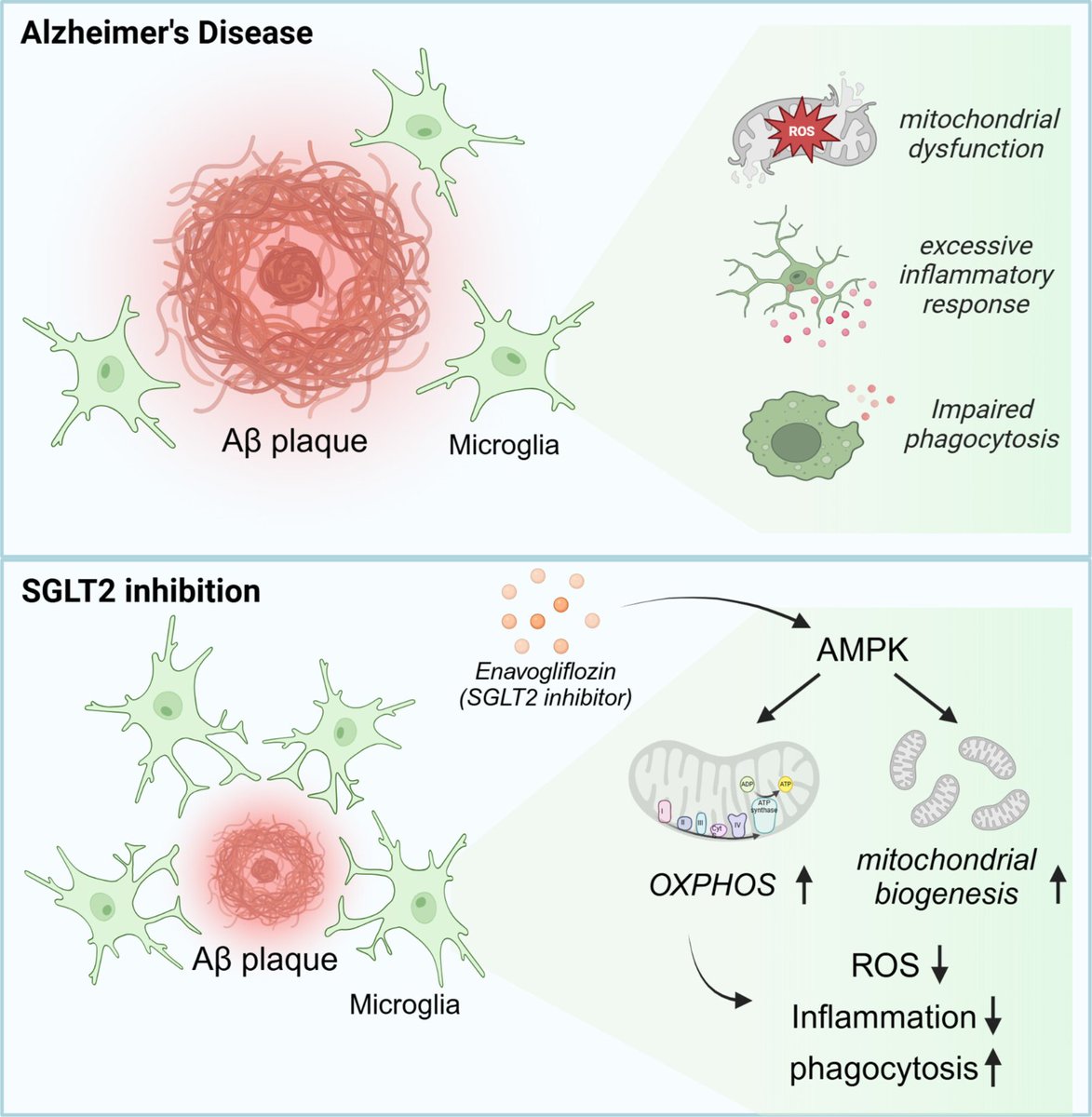
SGLT2 inhibitors (SGLT2i), widely used for glucose control and cardiorenal protection, are thought to act as caloric restriction mimetics, raising the possibility of anti-aging benefits.
- Preclinical studies suggested lifespan extension and reduced senescence burden with SGLT2i, but clinical data on aging biomarkers were lacking.
Study Design
-
Design: Multicenter, randomized, double-blind, placebo-controlled trial.
-
Participants: 150 patients with T2DM (142 completed).
-
Intervention: Henagliflozin 10 mg/day vs. placebo for 26 weeks.
-
Primary endpoint: Change in telomere length (peripheral blood leukocytes).
-
Secondary endpoints: IGF-1/IGFBP-3 system, glucose metabolism, β-hydroxybutyrate, immune function, metabolomics.
-
Trial registration: ChiCTR2300068127.
Key Findings
1. Telomere Length
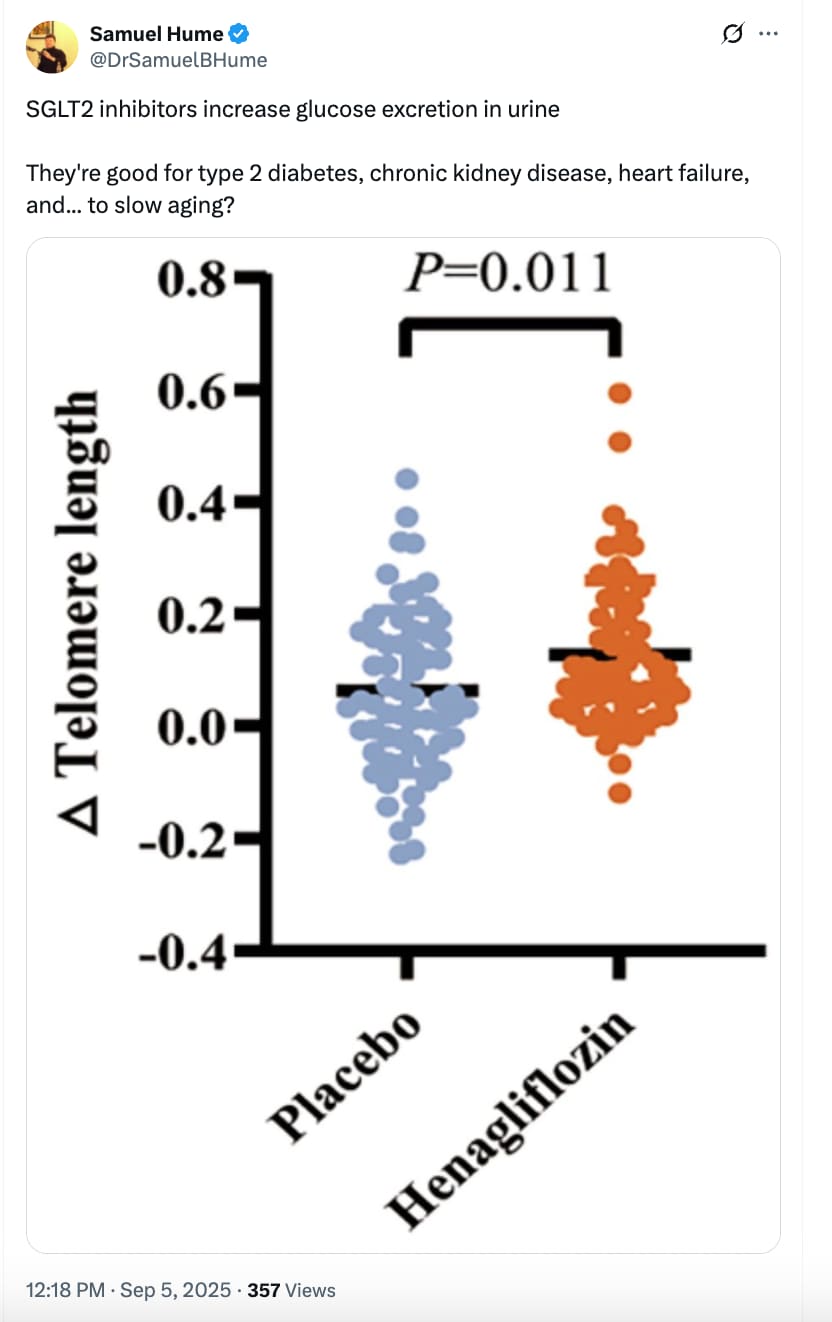
- Significant increase in telomere length in henagliflozin vs placebo (mean difference: +0.06 units; p = 0.011).
- 90.5% of treated patients showed telomere lengthening vs. 65.6% with placebo.
2. IGF-1 / IGFBP-3 Axis
- IGFBP-3 levels increased significantly (p = 0.013).
- IGF-1 and IGF-1/IGFBP-3 ratio tended lower (not statistically significant).
- Suggests a possible downregulation of GH/IGF-1 signaling, a pathway linked to lifespan extension.
3. Metabolic Outcomes
-
Improved glucose metabolism: lower fasting plasma glucose (−1.92 mmol/L vs −1.17 mmol/L; p = 0.030) and HbA1c (−1.37% vs −1.04%; p = 0.047).
-
Increased β-hydroxybutyrate (+0.05 mmol/L; p = 0.002).
-
Reduced body weight, BMI, and serum uric acid compared with placebo.
4. Immune Function
-
Granzyme B expression in cytotoxic T lymphocytes (CTLs) increased significantly (p = 0.033).
- Trends toward higher perforin expression in CTLs and T cells.
- No significant changes in inflammatory cytokines (IL-6, IL-10, IFN-γ).
- Suggests improved immune cell cytotoxic function (partial reversal of immunosenescence).
5. Metabolomics
6. Safety
- Well tolerated.
- Adverse events balanced across groups.
- Serious AEs occurred only in placebo group.
- No diabetic ketoacidosis (DKA) reported.
Discussion
-
Telomere extension is the first direct clinical evidence that an SGLT2i may influence an aging hallmark in humans.
- The IGF-1 axis modulation, ketone body increase, and immune enhancement parallel known effects of caloric restriction.
-
Thiamine metabolism emerged as a novel pathway, suggesting possible mitochondrial/energy-related anti-aging mechanisms.
- Results align with previous SGLT2i benefits in cardiovascular, renal, and frailty outcomes in older populations.
- Potential role as multi-system geroprotective agents, possibly complementary to GLP-1R agonists.
Limitations
-
Short duration (26 weeks) – no data on sustainability after discontinuation.
-
Single dose of henagliflozin studied.
-
Small immune-function sample size due to processing constraints.
-
Telomere length is a useful but imperfect biomarker of biological aging.
- No functional clinical aging endpoints (frailty, cognition, physical performance) assessed.
Conclusion
Henagliflozin (10 mg/day for 26 weeks) in patients with T2DM:
-
Extended telomere length,
- Improved glucose metabolism and ketone production,
- Modulated IGF-1/IGFBP-3 system,
- Enhanced cytotoxic T cell function,
- Induced favorable metabolomic shifts (↑ thiamine metabolism, ↓ sphingolipids).
This trial provides the first randomized clinical evidence of anti-aging biomarker modulation by an SGLT2 inhibitor, supporting their potential as geroprotective therapies.
=================================
Here’s a methods-first critique of the henagliflozin trial, focused on how convincingly it supports an “anti-aging” claim.
Bottom line
The study is a well-run, double-blind RCT that shows henagliflozin (10 mg/day, 26 weeks) favorably shifts several aging-adjacent biomarkers—notably leukocyte telomere length (primary endpoint), IGF axis components (↑IGFBP-3), ketones (↑β-hydroxybutyrate), selected immune cytotoxic markers (↑granzyme B in CTLs), and metabolomic pathways (↑thiamine metabolism; ↓PC/PE/sphingosine). However, the trial is short, single-dose, biomarker-only, with small mechanistic sub-samples and several analytic/methodologic caveats (surrogate outcomes, leukocyte composition, multiplicity, and untargeted ‘omics overfitting risk). The evidence is promising but preliminary for geroprotection; it does not yet demonstrate slowed biological aging or improved aging phenotypes.
Major strengths
-
Gold-standard design for pharmacology: multicenter, randomized, double-blind, placebo-controlled; 150 randomized (142 analyzed), balanced baseline characteristics.
-
A priori primary endpoint met: telomere length increased vs placebo (mean Δ difference ≈ +0.06; p = 0.011). Authors also re-checked the effect adjusting for smoking.
-
Convergent biological signals: IGF axis shift (↑IGFBP-3), metabolic changes consistent with SGLT2i/CR-mimetic physiology (↓FPG, ↓HbA1c, ↑β-hydroxybutyrate), immune cytotoxicity signal (↑granzyme B in CTLs), and coherent metabolomic pathway enrichment (↑thiamine metabolism; ↓immunosuppressive lipids). These point in the same directional hypothesis.
-
Safety profile: AE rates balanced; SAEs occurred only in placebo; no DKA reported.
Key limitations / potential biases
1) Surrogate focus and interpretability
-
Telomere length was measured in peripheral blood leukocytes and reported in relative units (qPCR-style), not base pairs nor calibrated to biological age models; no direct mapping to “years of aging” is possible. Short-term (26 wk) TL changes can reflect leukocyte subset shifts as much as true telomere elongation/attrition dynamics. While global WBC/lymphocyte/monocyte counts are shown (no between-group differences in changes), granular cell-composition adjustments (e.g., neutrophils, naïve/memory T, B, NK subsets) are not modeled for the TL endpoint. This tempers claims that the TL rise reflects slowed cellular aging.
2) Multiplicity and small mechanistic samples
- Multiple secondary/exploratory endpoints (IGF axis, cytokines, immune cytotoxic markers, metabolomics) were tested; no formal multiplicity correction is reported. Positive immune signals derive from a small subset (n≈ 15 placebo, 19 active), and metabolomics from 56 participants (32 active, 22 placebo) with 53 metabolites declared different at p < 0.05—raising false-positive risk without false discovery rate control. OPLS-DA is susceptible to overfitting if cross-validation/permutation testing isn’t rigorous (not detailed in the excerpt). Conclusions about mechanisms should be cautious.
3) Short duration and single dose
-
26 weeks, single 10 mg dose; no durability or dose-response. No post-discontinuation follow-up to test persistence or reversal of biomarker changes.
4) Aging outcomes not assessed
- No clinical aging phenotypes (frailty index, gait speed, grip strength, cognitive measures), no composite biological age clocks (e.g., GrimAge/PhenoAge), and no organ-specific function beyond routine metabolic labs. The study demonstrates biomarker modulation, not extended healthspan.
5) Missingness and measurement constraints
-
Body composition was analyzed in only n=22 due to equipment limits; lipid and blood-cell data have some missingness from site errors. The telomere assay and immune phenotyping required fresh blood at multiple centers—pre-analytical variability can creep in despite blinding. Details of TL assay reproducibility (intra-assay CV, calibrators) are not in the excerpt.
6) Generalizability and sponsorship
- Middle-aged T2DM cohort (mean ~52 y, China); unclear generalizability to older (>65), non-diabetic, or multi-morbid populations. The study drug was supplied by the manufacturer (no role in conduct per authors), which is standard but still worth noting in early-phase biomarker work.
Statistics & interpretation notes
- Primary analysis compares change-from-baseline between arms using t/Mann-Whitney tests; ANCOVA with baseline adjustment typically offers better precision and is often preferred for continuous endpoints. Authors did a smoking-adjusted sensitivity for TL; broader covariate-adjusted models could help.
-
IGF-1/IGFBP-3 ratio trended lower but was not significant; anchoring mechanistic claims (GH/IGF-1 suppression) on a non-significant ratio is suggestive, not confirmatory.
- Improvements in glycemia, BMI, and uric acid plausibly mediate favorable biomarker shifts; whether henagliflozin’s effects exceed what would be expected from any agent achieving similar metabolic changes remains untested here (no active comparator).
How convincing is the “anti-aging” claim?
-
Supportive: Pre-specified primary endpoint improved; multiple orthogonal biomarkers shifted in a direction consistent with CR-mimetic physiology; safety acceptable.
-
Not yet definitive: Lacks clinical aging endpoints, robust cell-composition controls for TL, multiplicity control for ‘omics/immune panels, longer follow-up, and dose-response. The findings are best framed as biomarker-level evidence of geroscience plausibility, not proof of slowed aging or improved healthspan.
What would strengthen the evidence (actionable next steps)
-
Longer, multi-dose, multi-center RCTs with post-drug follow-up to test durability/disease-agnostic benefits.
- Add epigenetic clocks (GrimAge, PhenoAge, DunedinPACE), proteomic clocks, and functional aging measures (frailty index, gait speed, grip strength, cognition).
-
TL measurement upgrades: flow-FISH or absolute TL (bp) calibration; explicit adjustment for leukocyte subsets (full differential and lymphocyte sub-phenotyping) in TL models.
-
Multiplicity control (FDR) and pre-registered analysis plans for ‘omics and immune panels; cross-validated OPLS-DA/permutation testing.
-
Active-comparator arms (e.g., GLP-1RA) or combination to test class-specific vs shared metabolic effects on aging biomarkers.
Overall verdict
A carefully executed, hypothesis-generating RCT that advances the field by showing consistent biomarker modulation in humans on an SGLT2 inhibitor. It provides encouraging, not yet conclusive evidence for anti-aging potential. Translation to clinical geroprotection will require longer, larger, and function-focused trials with rigorous biomarker methodology and multiplicity control.