I tend to agree. I suspect that perhaps the ezetimibe and bempadoic acid are making things a little more complex here, and perhaps resulting in misleading numbers. I ran out of Ez and BA recently and redid my blood tests and I’ve dropped (by this calculation) down to the 2nd level of risk (“low to moderate risk”)… but my LDL-C went from 46 to 89. I’d rather have the lower LDL-C…
1 Like
What does 0.6 monocytes represent? In my results, it is expressed as a percentage, which is required to make the calculation. Does 0.6 represent 60%
The equation needs absolute monocytes.
Mine -
My MHR calculated by ChatGPT5 (paid thinking mode.
Your MHR (using HDL = 53 mg/dL; absolute monocytes = 573)
- Convert HDL to mmol/L:
53 mg/dL × 0.02586 = 1.3706 mmol/L. NCBI
- Express monocytes in ×10³/µL:
573 cells/µL = 0.573 ×10³/µL.
- Compute MHR:
4.MHR = 0.573 ÷ 1.3706 ≈ 0.418*.
Answer: MHR ≈ 0.418 (unitless ratio, using monocytes in ×10³/µL and HDL in mmol/L).
Note: If your lab already reports “absolute monocytes” in ×10³/µL (e.g., 0.573), use that directly in step 2
I think the problem lies in using the correct units. Using the units you provided and plugging it into the formula results in=
To calculate MHR using the provided values:
Given:
-
Monocytes = 0.600 ×10³/µL
-
HDL = 53 mg/dL
Step-by-Step Calculation:
-
Convert HDL from mg/dL to mmol/L:
Formula: HDL (mmol/L)=HDL (mg/dL)×0.02586\text{HDL (mmol/L)} = \text{HDL (mg/dL)} \times 0.02586HDL (mmol/L)=HDL (mg/dL)×0.02586
53 mg/dL×0.02586=1.3706 mmol/L53 , \text{mg/dL} \times 0.02586 = 1.3706 , \text{mmol/L}53mg/dL×0.02586=1.3706mmol/L
-
Calculate MHR using the formula:
MHR=Monocytes (×10³/µL)HDL (mmol/L)\text{MHR} = \frac{\text{Monocytes (×10³/µL)}}{\text{HDL (mmol/L)}}MHR=HDL (mmol/L)Monocytes (×10³/µL)
MHR=0.6001.3706≈0.438\text{MHR} = \frac{0.600}{1.3706} \approx 0.438MHR=1.37060.600≈0.438
Final Result:
MHR ≈ 0.438
1 Like
To calculate MHR with the given values:
Given:
- Monocytes = 0**.42 × 10⁹/**L
- HDL = 95 mg/dL
Step-by-Step Calculation:
-
Convert HDL from mg/dL to mmol/L:
Formula: HDL (mmol/L)=HDL (mg/dL)×0.02586\text{HDL (mmol/L)} = \text{HDL (mg/dL)} \times 0.02586HDL (mmol/L)=HDL (mg/dL)×0.02586
95 mg/dL×0.02586=2.4517 mmol/L95 , \text{mg/dL} \times 0.02586 = 2.4517 , \text{mmol/L}95mg/dL×0.02586=2.4517mmol/L
-
Convert monocytes from ×10⁹/L to ×10³/µL:
0.42×109 cells/L=0.42×103 cells/µL=0.42 ×10³/µL0.42 \times 10^9 , \text{cells/L} = 0.42 \times 10^3 , \text{cells/µL} = 0.42 , \text{×10³/µL}0.42×109cells/L=0.42×103cells/µL=0.42×10³/µL
-
Calculate MHR using the formula:
MHR=Monocytes (×10³/µL)HDL (mmol/L)\text{MHR} = \frac{\text{Monocytes (×10³/µL)}}{\text{HDL (mmol/L)}}MHR=HDL (mmol/L)Monocytes (×10³/µL)
MHR=0.422.4517≈0.171\text{MHR} = \frac{0.42}{2.4517} \approx 0.171MHR=2.45170.42≈0.171
Final Result:
MHR ≈ 0.171
I don’t think your query to ChatGPT got the correct answer.
Using my query, your results are:
To calculate MHR with the given values:
Given:
-
Monocytes = 0.50 × 10³/µL
-
HDL = 50 mg/dL
Step-by-Step Calculation:
-
Convert HDL from mg/dL to mmol/L:
Formula: HDL (mmol/L)=HDL (mg/dL)×0.02586\text{HDL (mmol/L)} = \text{HDL (mg/dL)} \times 0.02586HDL (mmol/L)=HDL (mg/dL)×0.02586
50 mg/dL×0.02586=1.293 mmol/L50 , \text{mg/dL} \times 0.02586 = 1.293 , \text{mmol/L}50mg/dL×0.02586=1.293mmol/L
-
Calculate MHR using the formula:
MHR=Monocytes (×10³/µL)HDL (mmol/L)\text{MHR} = \frac{\text{Monocytes (×10³/µL)}}{\text{HDL (mmol/L)}}MHR=HDL (mmol/L)Monocytes (×10³/µL)
MHR=0.501.293≈0.386\text{MHR} = \frac{0.50}{1.293} \approx 0.386MHR=1.2930.50≈0.386
Final Result:
MHR ≈ 0.386
RapAdmin
#1038
But those numbers don’t seem to really make sense given the research study ranges (or we are all way high in the range, which seems unlikely):
Here is how my blood tests convey the monocyte measures:
From the Meng et al. study quartiles:
| Quartile |
MHR Range |
Interpretation |
| Q1 |
≤ 0.0064 |
Lowest risk |
| Q2 |
0.0065 – 0.0093 |
Low-moderate |
| Q3 |
0.0094 – 0.0144 |
Moderate |
| Q4 |
> 0.0144 |
Highest risk |
1 Like
LaraPo
#1039
Thus is what I get:
• Monocytes absolute: 0.42 ×10⁹/L
• HDL cholesterol: 95 mg/dL
Since MHR is a unitless ratio, you can directly divide:
\text{MHR} = \frac{0.42}{95} \approx 0.00442
 Why It Works
Why It Works
Even though monocytes are in \times 10^9/L and HDL is in mg/dL, the ratio is used as a relative marker, not a strict molar comparison. It’s meant to reflect the balance between inflammatory cells and anti-inflammatory lipoproteins, so the units are left as-is in clinical practice.
LaraPo
#1040
I also recalculated MHR for your numbers and got the following:
Let’s calculate your Monocyte-to-HDL Ratio (MHR) using the values you provided:
 Your Inputs
Your Inputs
• Monocytes absolute: 0.50 \times 10^3/\mu L = 0.50 \times 10^9/L
• HDL cholesterol: 50 mg/dL
 MHR Formula
MHR Formula
\text{MHR} = \frac{\text{Monocyte count}}{\text{HDL cholesterol level}} = \frac{0.50}{50} = 0.01
 Result
Result
Your MHR is 0.01
 Interpretation
Interpretation
An MHR of 0.01 is considered low, which generally suggests:
• Low systemic inflammation
1 Like
Here’s the lab report for monocytes. I have both a percentage and absolute numbers.
1 Like
Neo
#1042
@adssx do you how big the HDL effect is from flozinz? Do you think it’s helpful HDL up or just spurious (like the first gen CETP drugs seem to have perhaps been)
adssx
#1043
6 Likes
New treatment cuts cholesterol by nearly 50%, without statins or side effects
Inhibition of PCSK9 with polypurine reverse hoogsteen hairpins: A novel gene therapy approach
https://www.sciencedirect.com/science/article/pii/S0006295225002382?via%3Dihub
3 Likes
Davin8r
#1045
Just wanted to report that my insurance covers Nexlizet with NO prior authorization for $10/month ($25 for 90 days). I could have saved so much money by asking my doc years ago to “just prescribe it and see what happens”.
I figured for sure they wouldn’t do it since my LDL is already low and I’m on Repatha. Lesson is, don’t assume your insurance won’t cover it if you want to try bempedoic acid. And now I’ll be using the branded med rather than a foreign generic with the associated potential risks.
4 Likes
Consensus is that statins have a material effect on lifespan and healthspan.
Curious thoughts about this study that seems tl suggest they do for people who already have CAD but dont have a significant effect for those who dont.
So tear it apart 
https://www.jacc.org/doi/abs/10.1016/j.jcmg.2025.05.018?utm_source=signals.superpower.com&utm_medium=newsletter&utm_campaign=cholesterol-genes-drugs-cancer-clues-and-women-bodybuilders&_bhlid=25104835387f7d8d78d10130c3479b0ca0173506
Virilius
#1048
Which age group makes up the overwhelming majority of deaths from ASCVD? Old people.
Which age group already mostly has CAD? Old people.
Old people who don’t have any calcified plaque in their blood vessels already either have low LDL-C or are genetically protected from the negative effect of cholesterol through various mechanisms in which case statins don’t have much of an effect.
2 Likes
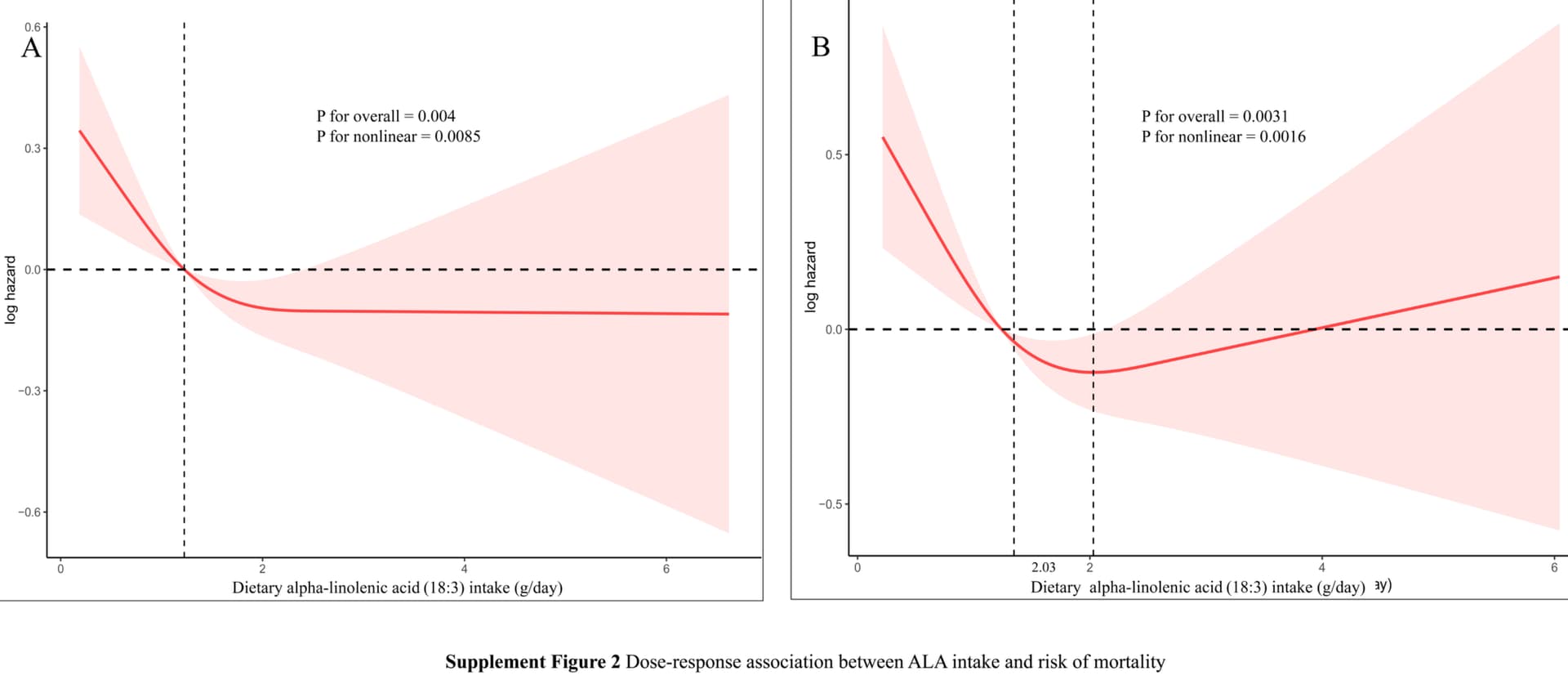
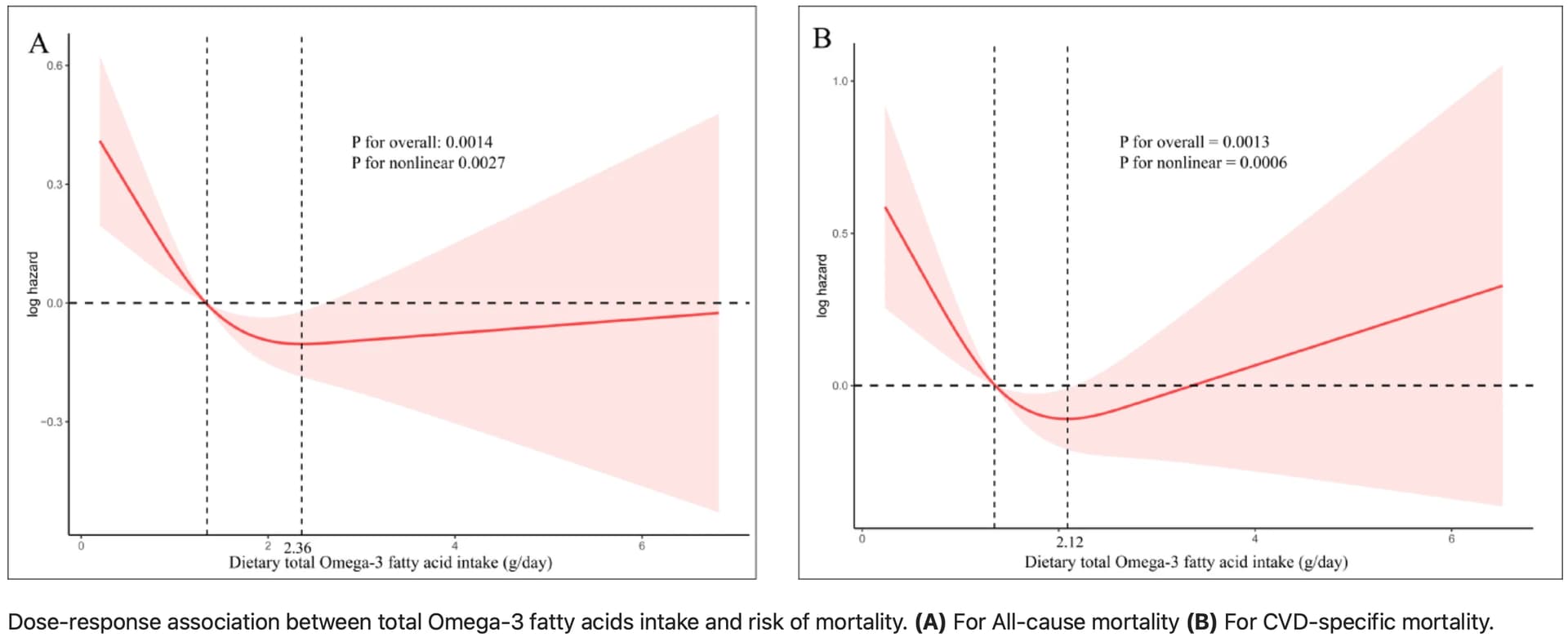
Association of dietary omega-3 fatty acids intake with all-cause and cardiovascular disease-specific mortality among individuals with cardiovascular disease
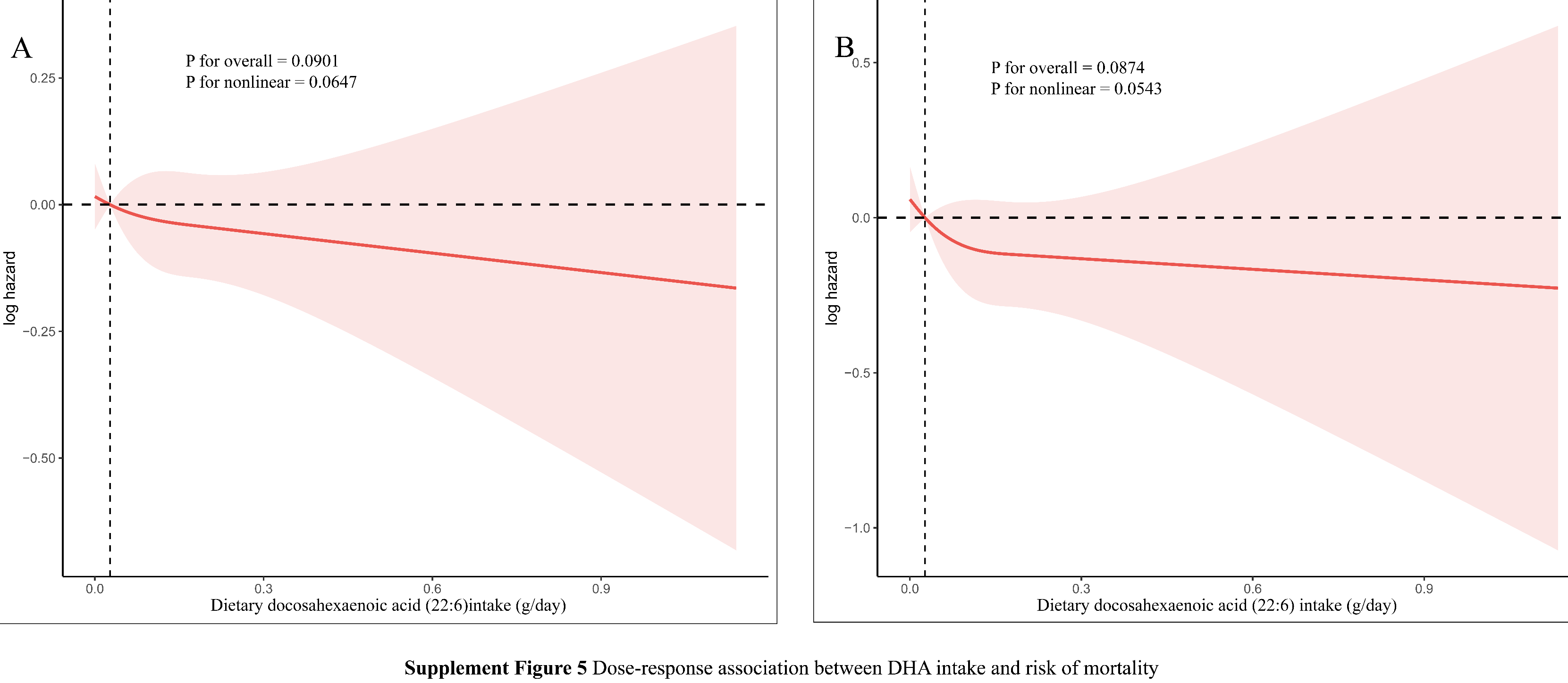
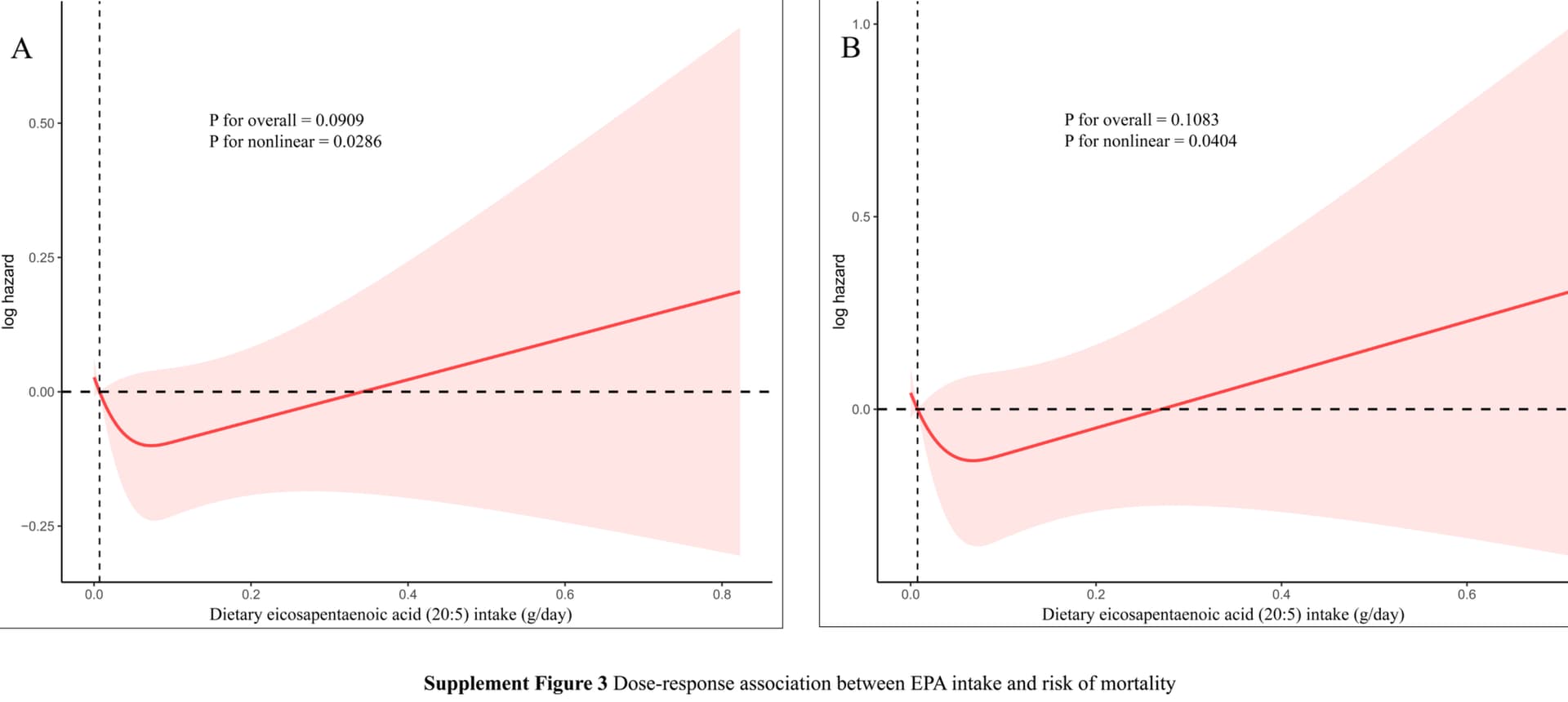
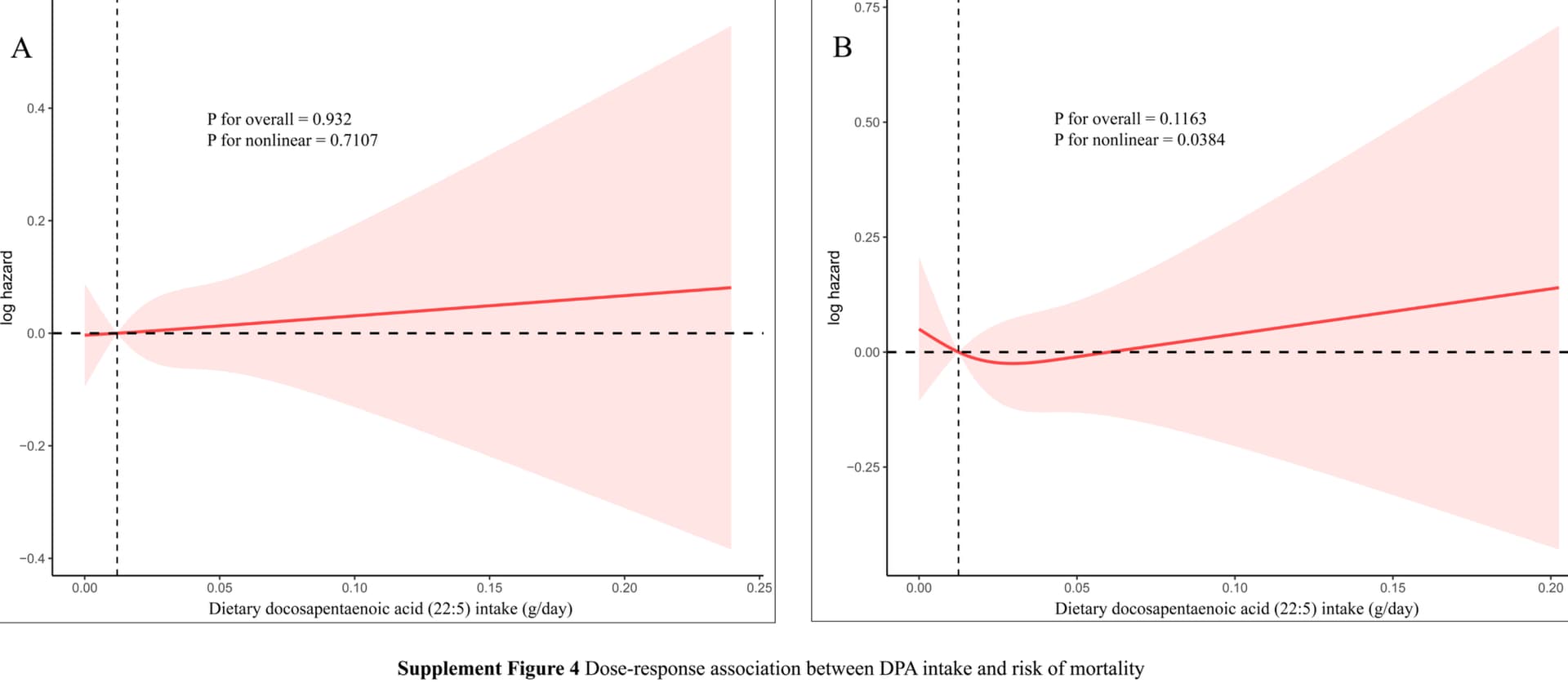
In the separate analysis of individual subtypes of the omega-3 fatty acid family, the consumption of alpha-linolenic acid (ALA) was obviously inverse-associated with CVD-specific mortality (HR of 0.64, 95% CI: 0.44–0.95). Nonetheless, the consumption of eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), and docosapentaenoic acid (DPA) did not show a significant association with mortality risk (P > 0.05).
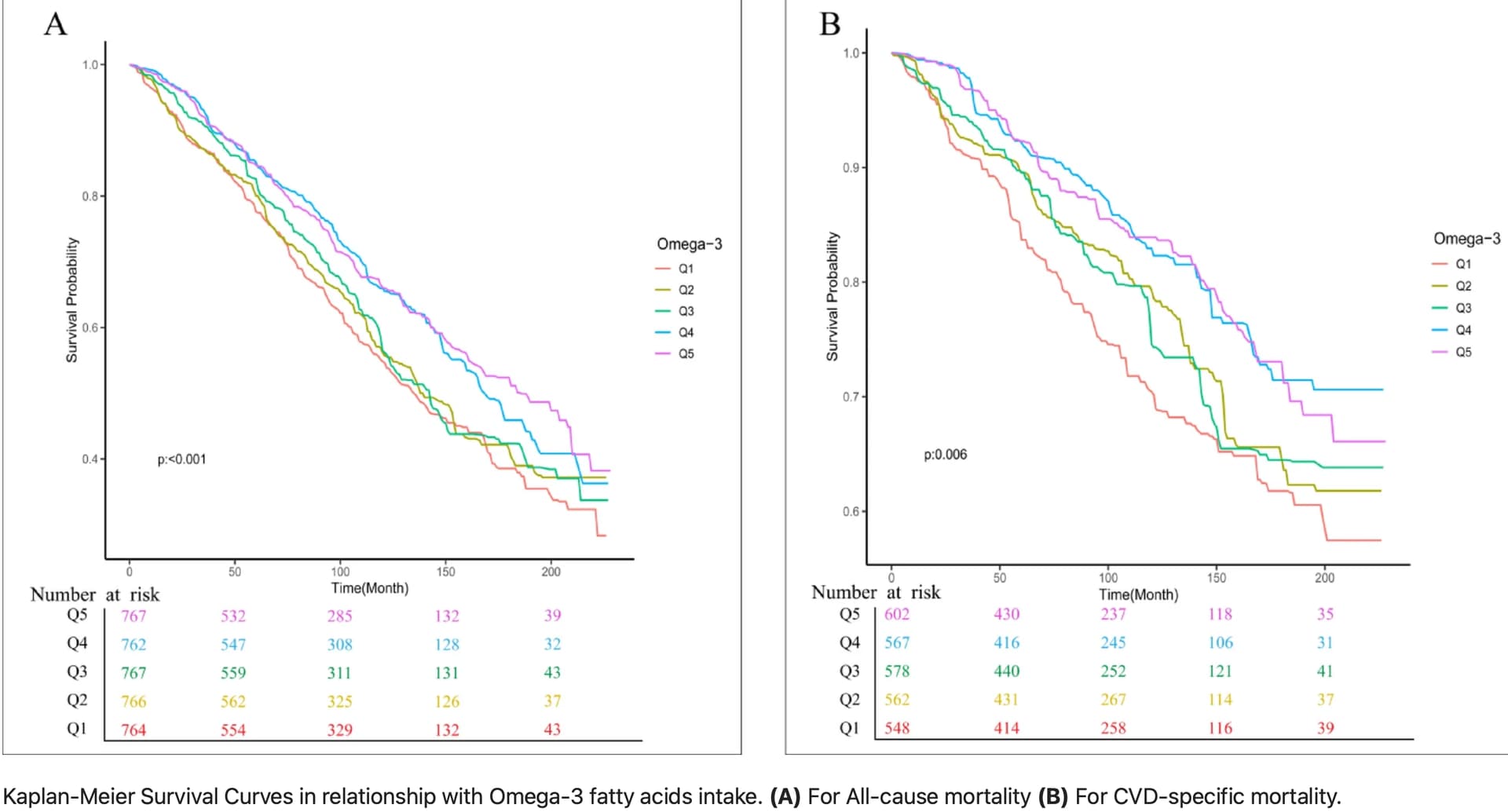
In the dose-response relationship analysis, total omega-3 fatty acid intake and ALA intake were observed to have an “L”-shaped nonlinear relationship with cardiovascular mortality, with the inflection points at 2.12 (g/day) and 2.03 (g/day), respectively. In summary, our research indicates that both total omega-3 fatty acids and ALA are inversely linked to the risk of all-cause mortality and cardiovascular mortality in patients with CVD.
We recommend a daily intake of 2.12 g of total omega-3 fatty acids, with an optimal intake of 2.03 g/day for ALA for CVD patients.
Open access paper:
https://www.nature.com/articles/s41598-025-21193-1
6 Likes
Does this mean we should swap out Omega-3 fish oil for ALA? I take 2 g a day of Omega 3 fish oil and I wonder if switching to ALA makes sense.
3 Likes
cl-user
#1052
Another data point for @adssx 's crusade against DHA.
EPA looks somewhat better
DPA not so good either
Surprisingly ALA is somewhat good.
Total Omega 3 are important though.
As confirmed by the KP plots.
4 Likes
LaraPo
#1053
It’s easy to get enough ALA by adding 1 teaspoon of chia seeds and 1 teaspoon of flaxseeds to your smoothie.
2 Likes