It seems my statin intolerance was worse than I expected. Even 5 mg of Atorvastatin daily caused muscle spasms in my calves and weakness in my thigh muscles. I have switched to 5 mg of Atorvastatin Mon-Wed-Fri. This is much better, and the spasms are gone along with most of the weakness. I guess only time will tell whether this schedule causes problems.
My LDL and ApoB without the statin is 68.
My LDL and ApoB with a daily 5 mg statin is 48.
So, maybe I can hit 55-60 with this new dosing regime? Thoughts?
3 Likes
RapMet
#1448
Never measured ApoB. Does it always equal LDL?
1 Like
My LDL and ApoB are the same at these low levels. When my LDL was higher (120) my ApoB was a bit lower (108).
1 Like
mccoy
#1450
NO, there is a thread about it (let’s see if I can find it), it hoovers usually in the range of LDL plus or minus 10 mg/dL, but there is no general rule.
Anyway, non-HDL is seemingly the best proxy for ApoB
3 Likes
adssx
#1451
And if you don’t have access to apoB you can calculate eLDL-TG by yourself and eLDL-TG is apparently even better than apoB, LDL-C and non-HDL-C:
2 Likes
A_User
#1452
I find it unlikely it’s better than apoB because of an association study, also a marker that might be partly elevated by obesity or insulin resistance is of no use to me who don’t have that. There’s confounding.
adssx
#1453
I haven’t checked the rest of the literature, but I still think that with LDL-C, non-HDL-C, and the ability to calculate eLDL-TG, people don’t absolutely need apoB if it’s not included by default in their usual package. Of course, if they can have it, they should go for it.
2 Likes
A_User
#1454
I don’t think so, because it’s most likely a worse marker. Your eLDL-TG can be okay but your apoB terrible, and then you’re getting ASCVD since the latter is causal and the former just association with confounding.
It might simply be testing for obesity and insulin resistance, for example. Just because you’re not that because they increase risk doesn’t mean you’re fine. This is a common trick people use to justify suboptimal apoB, as well, even though it’s their own health.
adssx
#1455
Do you have a source? Dr Lipid claims that it’s been known for 20 years that LDL-TG is better than LDL-C. I haven’t checked the literature.
I can’t think of a situation where LDL-C AND non-HDL-C AND eLDL-TG are “okay” and apoB is “terrible”.
Again: if you can easily get apoB, do get it. If not, LDL-C, non-HDL-C, and eLDL-TG will do the job.
A_User
#1456
I meant compared to apoB.
If your LDL-C, non-HDL-c, and eLDL-TG are all in the 5th percentile, then that’s perfectly good. Using solely anything that is based on association, with confounding with obesity or insulin resistance is a bad idea, is my point. Why it can’t replace apoB.
1 Like
adssx
#1457
5 Likes
As a layman, I really don’t understand this paper.
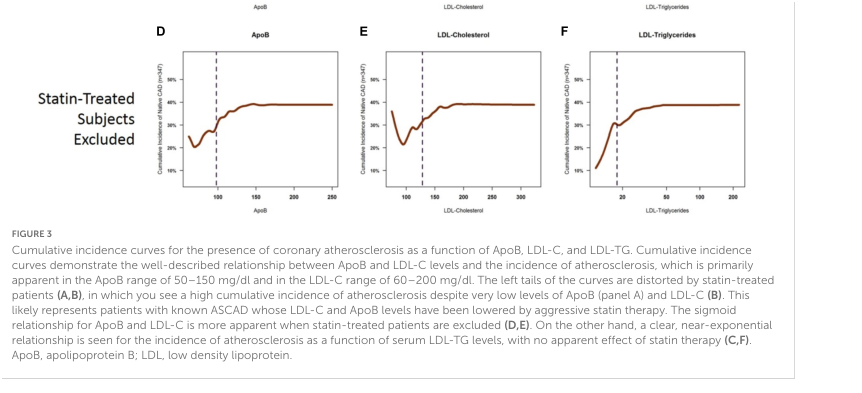
“The left tails of the curves are distorted by statin-treated patients (A,B), in which you see a high cumulative incidence of atherosclerosis despite very low levels of ApoB (panel A) and LDL-C”
“On the other hand, a clear, near-exponential relationship is seen for the incidence of atherosclerosis as a function of serum LDL-TG levels, with no apparent effect of statin therapy (C,F). ApoB, apolipoprotein B; LDL, low density lipoprotein.”
Is this another indicator that statins are probably worthless?
Also, I don’t understand the relationship of LDL-TG
What is the number we want to achieve?
Often, the LDL-TG will be a negative number.
On the other hand, a person with a low TG number would have a positive number.
Your help in understanding this paper would be appreciated
3 Likes
RapAdmin
#1459
I hope this has not been posted already:
Covid Can Raise the Risk of Heart Problems for Years
People who had severe infections are especially vulnerable.
https://www.nytimes.com/2024/11/22/well/covid-heart-health.html?unlocked_article_code=1.cE4.dp4R.HbLsbyPiY4pN
This article reviews a large US study that found the more times someone gets infected by COVID variants, and the more severe their symptoms, the higher their risk of developing chronic heart disease.
A person submitted a comment (below) about the role of endogenous CO in causing this heart disease and suggest COVID survivors can lower this and other CO- related risks by donating blood or phlebotomy.
Ironically, the best defense against getting a severe case of COVID or any other respiratory virus is to smoke a cigarette or a pipe at the first sign of infection, inhale deeply, and hold your breath for 10 seconds before exhaling.
The high level of CO in smoke is anti-viral, which is why smokers worldwide had lower than expected rates of COVID-19 infection, hospitalization and death.
They were only 1% of cases in US hospitals in 50 states vs 14% expected, based on a CDC report published in MMWR in April 2020. Subsequent studies from dozens of other countries showed smoking was highly effective against all COVID variants, reducing risk by over 95%, which is way better than any COVID vaccine ever achieved.
Although smokers are better protected from viral infections by their chronically high CO levels, they pay a high price with higher rates of heart diseases, non viral lung diseases such as emphysema, and cancers.
2 Likes
Virilius
#1460
I am also down to 20mg atorvastatin/day taken at night as I suspect some interaction with one of my other supplements/meds that I take in the morning. Ubiquionol is taken once a week at a low dose to replenish any inhibited CoQ10. This seems to keep side effects low.
1 Like
Please help me understand what this paper means.
I believe LDL-TG refers to “Low density lipoprotein triglycerides,” which is the amount of triglycerides found within low-density lipoprotein (LDL) particles in the blood.
My understanding of what you quoted from the paper is:
- ApoB and LDL are positively correlated with atherosclerosis if you’re not taking statins (higher ApoB → higher atherosclerosis). Though looking at the chart, there seems to be a sweet spot somewhere between 75-125 for LDL and 50-100 for ApoB
- If we add the cohort of people that’s on statins, there’s a high incidence of atherosclerosis at low ApoB and LDL. The authors believe that’s because some people are on aggressive statin therapy because they already have atherosclerosis, i.e. the high atherosclerosis came before the statins and resulting lower ApoB and LDL.
- LDL-TG is the most direct indicator of atherosclerosis. The relationship is quite impressive, almost a perfect predictor.
Does anyone know of any blood test that measure LDL-TG? And any remedies to keep it low?
3 Likes
My mother had low LDL (38) but high Triglycerides (240). She had a heart attack and stroke. Low LDL is not enough. She is also diabetic 8.8 HBA1C. I believe the diabetes and triglycerides (from all the wrong foods) caused her heart attack and stroke. Luckily she had very quick treatment so the damage was minimized. She had the heart attack while her heart was being monitored in the hospital.
6 Likes
mccoy
#1465
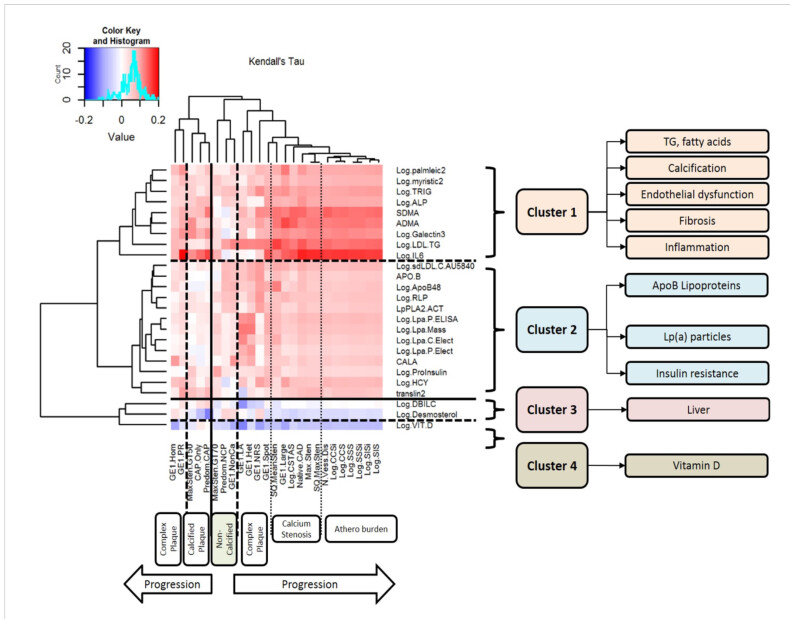
The article sure is not an easy one to understand. Graph 1 is clear enough though, the markers with higher positive correlation with ascertained ASCD (by imaging plaque measurements) are those in cluster 1= DA, AMDA, Log.IL6 mainly. but even the other markers, i cluster 1, exhibit some positive correlation.
Then there is the pretty clear explanation in the conclusions.
A key finding was that, out of tens of thousands of
blood-based molecules and biomarkers, LDL-TG emerged with
a potential central role in human coronary atherosclerosis,
potentially as a function of abnormal hepatic lipase activity.
This was seen in our hypothesis-free, causal, Bayesian network
analysis, which included 24,929 variables and 110,350 significant
edges in the models. LDL-TG was directly connected to human
coronary atherosclerosis in 95% of the models in the ensemble.
As a comment, OR is about the same as HR, the LDL-TG shows a more congruous trend, with small ORs at very small LDL-TG quantities
1 Like