O3:
1. Tidied transcript (edited for readability, filler words and ad‑breaks removed)
Intro (0 – 2 min)
I’m starting to wonder if I’m oversharing. You already have my blood tests, sperm results, CT‑angiogram… and now you’re getting my biological‑age report. I just received a panel of 100‑plus biomarkers from Function Health and a few things jumped out, including one blind‑spot even I’d missed. I’m sharing the full results because data and transparency help us all—whether that means lifestyle tweaks, supplements, or a chat with your doctor.
What we’ll cover
- Hormones (testosterone, oestrogen, FSH, LH)
- Nutrient status (with one surprise deficiency)
- Thyroid health
- Cardio‑metabolic markers (Apo B, glucose) & environmental toxins
- My biological age (using Dr Morgan Levine’s PhenoAge clock)
Hormones & fertility (2 – 8 min)
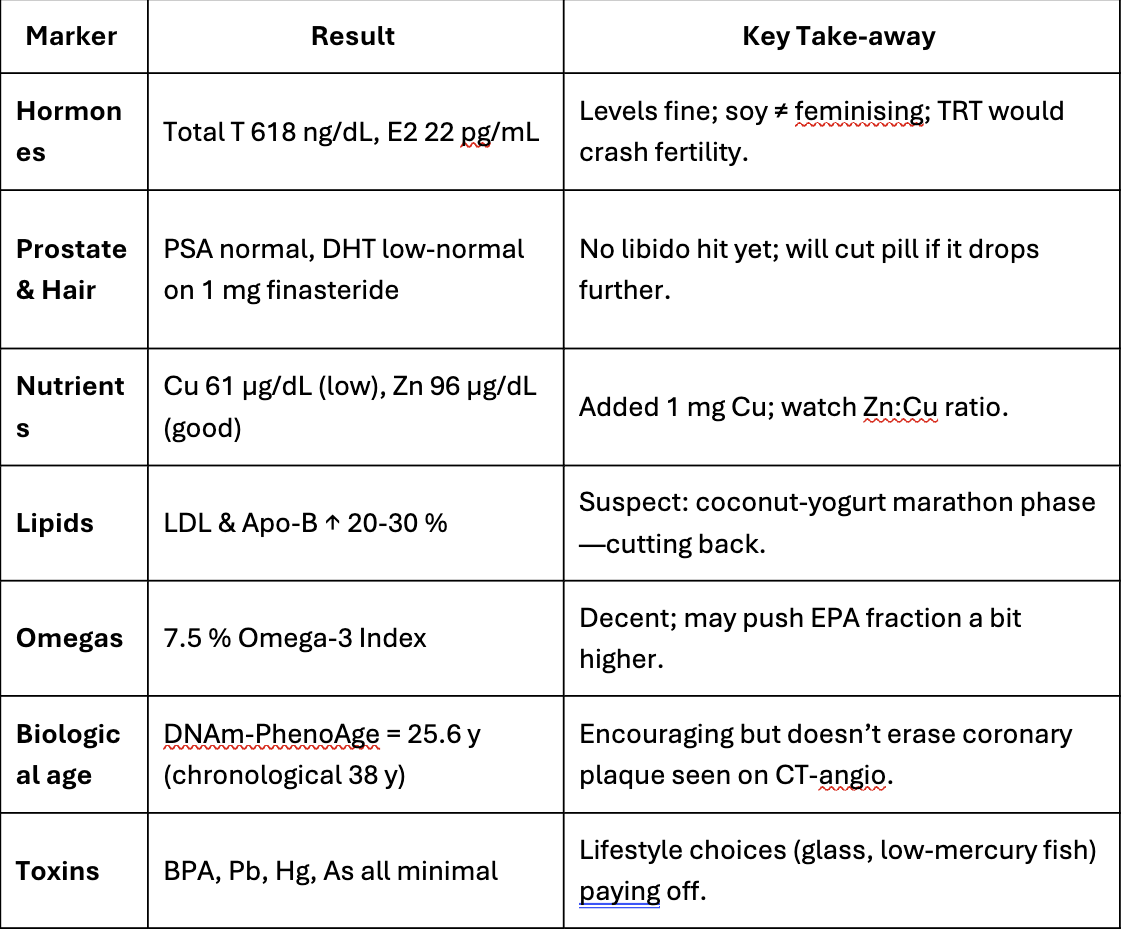
- Estradiol‑2: 22 pg/mL—well inside the male range (10‑40). Soy doesn’t “feminise” men; meta‑analysis of 38 RCTs confirms no effect on testosterone or oestrogen.
- Total T: 618 ng/dL, free T: 108 pg/mL—both healthy. No need for testosterone‑replacement therapy (TRT) when levels and energy are good.
- HRT shuts down endogenous T and sperm production, risking infertility. My FSH (6.9 IU/L) and LH (4 IU/L) are normal, matching last year’s favourable semen analysis.
- Clip with urologist Dr Ramy Ghayda: exogenous testosterone often drives sperm count to zero; 15–20 % of men never recover testicular volume.
Prostate & DHT (8 – 14 min)
- PSA panel all normal.
- DHT low‑normal—expected, because I started 1 mg finasteride for hair‑loss. Side‑effect (reduced libido) hasn’t appeared; if DHT drops too much I’ll halve the dose.
Nutrient panel surprises (14 – 22 min)
- B‑12 (via MMA & homocysteine) and vitamin D (57 ng/mL) solid.
- Omega‑3 “omega‑check” 7.5 % (EPA 2.5 %, DHA 3.3 %, DPA 1.6 %).
- Iron: Hb 15.7 g/dL; ferritin 39 ng/mL (low‑normal) but saturation 44 %.
- Zinc good (96 µg/dL) but copper low (61 µg/dL). Likely linked to zinc supplementation competing for absorption; I’ve switched to a multi with 1 mg copper.
- Magnesium, iodine, selenium all fine.
Thyroid & cardio‑metabolic (22 – 25 min)
- TSH, free T3/T4 and antibodies normal.
- Glucose, insulin, HbA1c perfect; CRP very low.
- Weak spot: LDL‑C and Apo B up ~20–30 %—probably the coconut‑yoghurt phase while marathon‑training. I’m sensitive to lauric‑acid saturated fat.
Environmental toxins (25 – 27 min)
Aluminium, arsenic, BPA, lead, mercury all minimal; BPA undetectable.
Biological age (27 – 29 min)
DNAm‑PhenoAge estimate: 25.6 y— ≈13 y younger than my calendar age. Encouraging, but not a free pass; my CT‑angiogram shows early plaque, so LDL/Apo B remain priorities.
Take‑home messages (29 – 33 min)
- Annual labs + regular blood‑pressure checks catch issues early.
- Health is dynamic; address weak links before they snowball.
- Grateful for the privilege of access—aim is to normalise preventive care.
(Full 33‑minute verbatim PDF is in Simon Hill’s show‑notes.)
### 2. Executive summary
-
Overall the host, Simon Hill, reports broadly favourable bloodwork: robust sex‑hormone profile, strong nutrient status, excellent glycaemic control and inflammation, minimal toxin exposure, and a “younger” biological‑age score.
-
Red flags: slightly elevated LDL‑C and Apo B—likely diet‑induced—and an unexpected copper deficit (possibly from excess zinc).
-
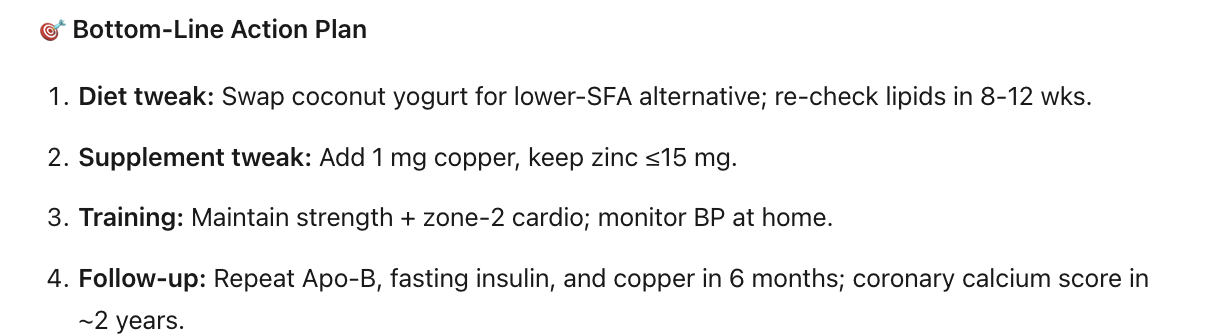
Key interventions he plans: reduce coconut‑derived saturated fat, tweak omega‑3 dosing, add 1 mg copper, continue strength/endurance training, monitor labs and blood pressure.
-
Educational points: clarifies myths around soy and hormones, cautions against indiscriminate TRT, highlights finasteride’s pros/cons, and stresses routine screening for silent risks like hypertension.
### 3. Critique
| Aspect |
Strengths |
Caveats / Limitations |
| Transparency & structure |
Shares raw PDF, walks viewers marker‑by‑marker, explains physiology clearly. |
Partnership with Function Health is disclosed but still a marketing tie‑in; viewers may conflate educational content with an ad. |
| Hormone discussion |
Correctly notes that normal testosterone + good symptoms ≠ need for TRT; highlights fertility suppression with exogenous T—consistent with clinical reviews. (PMC) |
Omits mention of alternative treatments (e.g., clomiphene, hCG) for symptomatic men who want fertility. |
| Finasteride segment |
Gives real‑world DHT data; quotes sexual‑side‑effect prevalence (≈1.5–4 %). (PMC) |
Underplays “post‑finasteride syndrome” reports; incidence is low but consequences can be severe and longer‑lasting in some cases. |
| Nutrient insights |
Makes a useful point about zinc competing with copper and immediately adjusts supplementation. (Medsafe) |
Copper measured once; without ceruloplasmin or repeat testing it’s hard to know if this is chronic or transient. |
| LDL/Apo B rise explanation |
Correct that lauric acid (coconut fat) can raise LDL. (The Nutrition Source) |
The claim that his spike is “20–30 % from coconut yogurt” is plausible but unverified without a controlled diet or repeat lipid panel. Other factors (training stress, weight change) not explored. |
| Biological‑age reporting |
Uses Dr Levine’s DNAm PhenoAge clock and clarifies it’s research‑grade. (PMC) |
PhenoAge is validated for population risk, not individual diagnosis; a 13‑year “bonus” can fluctuate several years between draws. May give false reassurance. |
| Take‑home advice |
Emphasises affordable, high‑impact checks (blood pressure) and lifestyle before meds; balanced. |
Cost of 160‑marker panels (~US $499/year) may be prohibitive; benefits over a standard evidence‑based panel are not discussed. |
Bottom line
Simon Hill delivers an engaging, largely evidence‑aligned walkthrough of his labs and uses them to illustrate practical preventive‑health principles. The episode shines in demystifying biomarkers and cautioning against trendy but unjustified interventions (e.g., elective TRT). Viewers should, however, remember:
- One lab snapshot is not destiny—repeat testing and clinical context matter.
- Biological‑age “clocks” are promising but still experimental; track trends, not single numbers.
- Comprehensive panels and devices marketed direct‑to‑consumer can be helpful if you understand their limits, but the essentials (blood pressure, lipids, HbA1c, kidney/liver panel) remain the highest‑yield for most people.
As always, interpret any abnormal result with a qualified clinician—not just a colourful dashboard.
Sources
(theproof.com, PMC, PMC, The Nutrition Source, PMC, Medsafe)

 | The Proof Podcast EP #373")