What you’re refering to is a trend with a p value of 0.06-0.15 or so. A p value of 0.43 is meaningless noise.
adssx
#393
Yes but the absence of any trend towards ACM reduction is disappointing after 5y of use in a large trial.
3 Likes
L_H
#394
Yes but the absence of any positive sign of ACM benefit is disappointing after almost 5 years. It’s a large trial and well over a third of deaths are from cvd in that cohort. So the fact that acm is numerically higher in the ezetimibe group is… “disappointing”
2 Likes
A_User
#395
It wasn’t a blinded placebo-controlled trial.
L_H
#396
“Our trial has several important limitations. First, this was a prospective RCT with blinded outcome assessment, but not a blinded placebo-controlled trial. We could not use matching placebo as control because of cost considerations. We consider that this determination is acceptable because most of the outcomes were objective variables and were analyzed by the event evaluation committee in a blinded manner.”
This logic makes sense to me given that the outcome we’re talking about is death. It’s unlikely that the lack of placebo-controlled blinding could have caused the control group to avoid death somehow? Or alternatively caused the ezetimibe group to die?
Bicep
#397
The blue line is above the red line the whole way, a little more so after a couple years.
I’m no statistician but did have a couple courses in grad school. It was about 40 years ago so I’m not digging out the book, but I know what wee p is.
You can have it. I started taking it after my last bad news, but it’s back on the shelf. If they weren’t screwing us so bad I’d double up the fatty 15.
Yes, but with a p value of 0.43 that is very, very likely just due to random chance. If the p value were below 0.05, it would be statistically significant. If it were anywhere from 0.06-0.1X, it could be called a trend.
What this data tells me that ezetimibe, my itself, likely doesn’t have an effect on acm at all. I will still take it in addition with rosuvastatin though.
3 Likes
Bicep
#400
You’re paying money for something that will kill you sooner. Big picture.
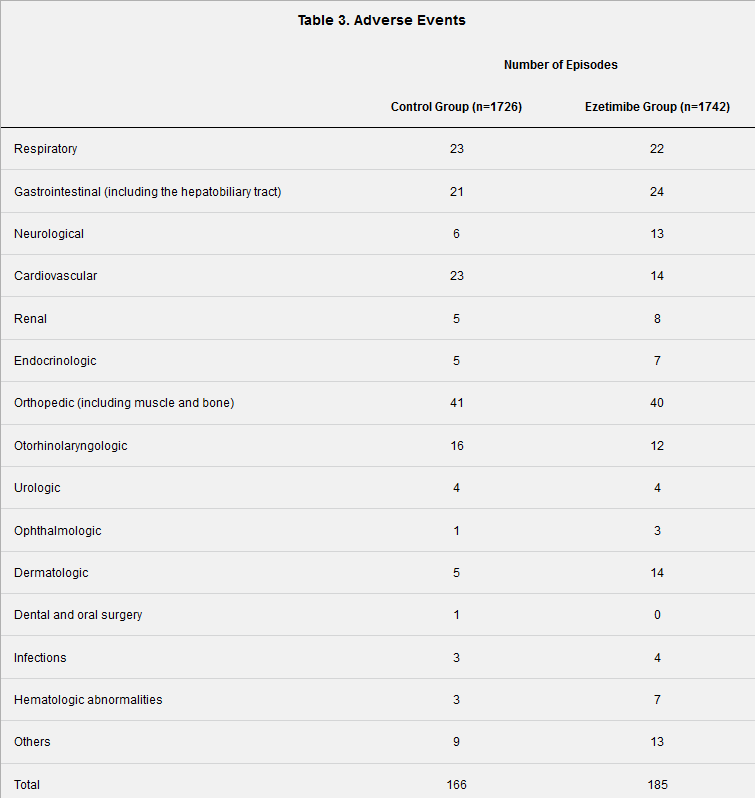
More than double the adverse neurological events
Almost double the renal adverse events
Almost triple the dermatologic adverse events
More than double the hematologic events
It loses on adverse events, it loses on all cause mortality. Thank you @adssx for posting this.
Not statistically significantly so, not even trending towards it. Besides, when it came to the statistically significant rosuvastatin acm reduction in the JUPITER trial, many people opposed to controlling their cholesterol ignored that too or claimed that the lines were converging by year 5 (they weren’t).
Neo
#403
1 Like
adssx
#405
Question to the statin and LDL skeptics: What do you think are the most important things to measure and control to prevent CVD, especially atherosclerosis? Which levels are optimal? Which treatments do you recommend? Is it just that you consider ApoB a bad metric for CVD risk?
I ask this because when I read LDLSkeptic’s tweets, it looks like even he agrees that sdLDL and Lp(a) are important:
But he considers that glycemic control and insulin sensitivity are as important (if not more?):
Glycemic control does seem to be an important factor. My mother’s heart attack seems to be predicated on her diabetes and high BP. Inflammation and LDL (ApoB) are also very important. In the end, it’s not just one factor but a confluence of many. My mother had near optimal LDL (110) yet still had two stents put in due to blockages in her arteries. Her ApoB was also near optimal.
You can’t just hit one factor. You need to address the core key ones.
3 Likes
adssx
#407
I agree with you: hence my question, according to the “anti ApoB” crowd, what are the core key ones?
1 Like
A_User
#408
Optimal LDL isn’t around 100, optimal is below the 5th percentile or lower as a proxy for apoB.
And all of the other factors are very important as well, of course, but they do not protect against atherosclerosis in the first place. If someone already has atherosclerosis they need to decrease all other risk factors which is important either way.
2 Likes
I agree that 110 isn’t optimal. But on the Johns Hopkins cholesterol chart, 100-120 is 'near optimal '.
I’d view 60 as optimal.
1 Like
A_User
#410
No, 60 is not optimal as shown in the clinical trials for high risk patients using PCSK9i + statin where they decrease median LDL to the 20’s and still show a reduction in events etc.
I see all the other risk factors as an amplifier of lifetime exposure to LDL. If you have extremely low apoB throughout life they don’t matter for heart disease as you cannot multiply risk without enough exposure. That’s why extremely low apoB levels are so important.
To say you can’t hit one factor is wrong as the genetic studies show the people with low levels throughout life are protected from disease. It’s wrong to assume that level is the same as medical recommendations and includes time of exposure.
5 Likes
50-60 is optimal for those with not a lot of risk factors imo. Those with multiple risk factors should aim for below 40.
1 Like
Bicep
#412
It came from the study you provided and I know the study was not powered to prove anything except that it reduces cardiac death, but the curve is suspect and it did lose in adverse events:
1 Like
adssx
#413
Thanks. Doesn’t look great indeed. Although they don’t mention what these adverse events are. Is it just a mild headache or dementia onset?
2 Likes