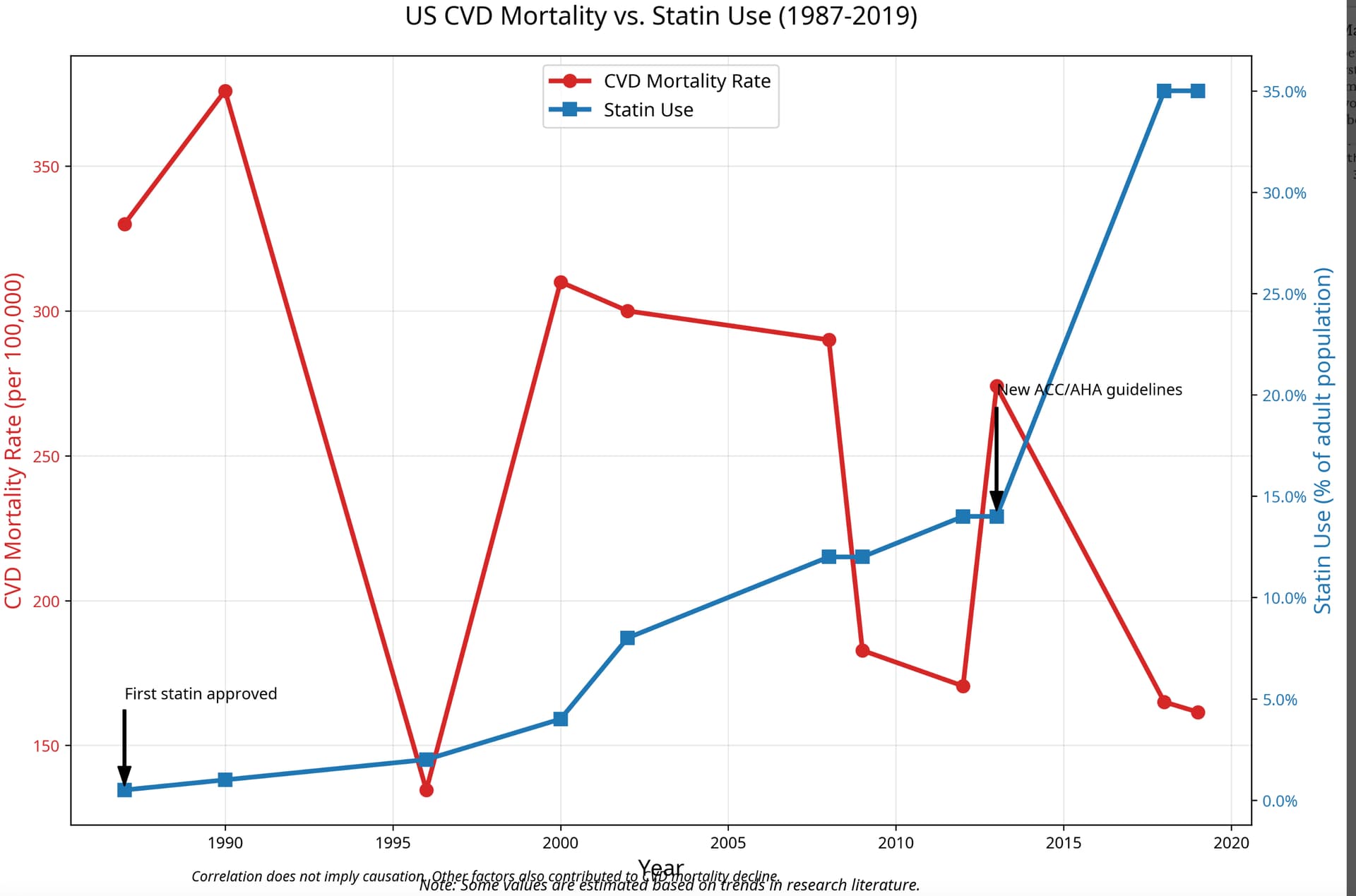
Looking at these graphs of CVD mortality rates, I thought again about my very favorite public health intervention program - The North Karelia Project. I think it is super interesting, in that the numbers from the graph AnUser posted match very closely the Finnish numbers. In 1980, the CVD death rates for males in the USA was roughtly 507/100K. In Finland CVD deaths in the late 60’s, early 70’s was about 500/100K - in the famous Ancel Keys Seven Countries Study, Finland had the worst statistics. Finland during that period of time had the highest rates of death from heart attacks in the world. It is quite sobering to consider that present day USA has CVD mortality rates on a similar level, and here we are, in the 2020’s where you’d think we’ve learned our lessons. In the North Karelia province of Finland, the rates were an astronomical 700/100K during the late 60’s early 70’s. There were many factors epidemiologists, physicians and health officials zeroed in on: cholesterol levels, smoking and blood pressure. Finland had the highest cholesterol levels on a population level recorded in any country. Notably, Finland reached the 500/100K CVD mortality rates with smoking rates dramatically higher than current smoking rates in the USA - which tells us, that the risk factors in the USA leading to the current horrendous CVD mortality rates must be somewhat different than in Finland of that era. We managed to get to 500/100K despite much lower smoking rates - quite an “accomplishment”.
The North Karelia Project is a gold mine of data and a stellar example of an extremely successful public health intervention - it is the finest achievement in lowering CVD death rates by public policy anywhere in the world, at any time. When I see endless arguments about cholesterol or diet - I just think of the North Karelia Project, which is a direct refutation of so many talking points by various folks when it comes to cholesterol and diet.
The North Karelia Project: Cardiovascular disease prevention in Finland
I give a quotation below, but really the whole paper is worth reading, it is so rich in data! For that matter it is worth buying books about this - for anyone interested in the subject of CVD health, this is absolutely wonderful reading.
"Serum cholesterol level and diet
Before the 1970s North Karelia was a poor, rural area. Small farming and forest industry were the main occupations. After the Second World War, the living standard started to improve rapidly. The dairy industry developed and people had enough food to eat. Dairy products were highly valued and a high intake of butter, cream, full milk, and cheese was regarded especially healthy. It was, therefore, painful to recognize that this diet seemed to be one of the main reasons for high mortality rates from cardiovascular diseases. The following advice was given to the population5:
-
use low-fat milk, non-fat milk or sour milk instead of high-fat or whole milk
-
use other low-fat dairy products instead of high-fat products
-
cut down the amount of butter or margarine on bread and change to soft margarine or soft butter (mixture of butter and oil)
-
cut off visible fat in meat, choose lean meat and sausages, and prefer fish and poultry
-
prepare food without adding extra (animal) fat, in cooking prefer boiling and baking
-
use vegetable oil in salad dressing and when baking
-
restrict the use of eggs (egg yolk) to only a couple per week
-
increase intake of whole-grain cereals
-
increase consumption of vegetables, roots, berries and fruits
Most of these original recommendations are still valid in Finnish society. Hard margarines have almost disappeared after the role of trans fats was discovered in the 1980’s. At present, soft butter contains mainly butter and very little oil. Soft margarines are recommended nowadays instead.
The nutritional messages were spread through different channels and in connection with different activities in the community. During the original project period (1972–1977) a total of 342 newspaper articles were published, in addition to 769 articles dealing with other risk factors, over 100,000 leaflets were distributed. Hundreds of training seminars were organized for healthcare workers, mass catering personnel, and the general public. Diet was discussed in 167 health education meetings attended by 12,100 participants. Local housewives associations (the Martha Association) organized 344 special “parties of long life” in local villages where healthy food was cooked and served to village members. Over 15,000 people participated in these meetings. Special training meetings were organized to change the diet in mass catering at workplaces, schools, hospitals and restaurants.
On a national level, since the 1980’s, several sectors became involved. National dietary guidelines were published for the first time in 1981 by the National Nutrition Council. A national cholesterol consensus meeting was held in 1989. Guidelines on prevention of coronary heart disease in Finland were published in 1987, together with national health authorities and voluntary organizations. Since then, these documents have been updated regularly.
Government became more involved and gave a health policy statement in 1985 where the role of healthy nutrition as an important goal was recognized. The law on dietary fats in 1987 allowed mixing dietary fats and oils to make new types of products available. The Finnish food industry has, with increasing health consciousness of consumers, been very active in developing new low fat products. In addition to low fat milks and spreads, low fat cheese, ice cream, sausages etc have appeared in the markets. Later, margarine with plant sterols was developed. A new variety of rapeseed oil was developed and it became widely used in homes and the margarine industry. Many voluntary organizations have also been very active, especially the Finnish Heart Association. Large-scale public health campaigns were organized in mass media. Health issues also became an important topic in magazines, newspapers and TV and radio programs.
Serum cholesterol reduced in North Karelia between 1972 and 2012 from 6.92 mmol/l to 5.46 mmol/l (−21%) in men and from 6.81 mmol/l to 5.37 mmol/l (−21%) in women5. In men, serum cholesterol level reduced more in North Karelia than in the reference province Kuopio during the first five years from 1972 to 1977. Since then, the development in serum cholesterol level has been very similar in different parts of the country (Figure 2). Saturated fats reduced from 20% of energy intake to 12% in 2007, and increased from 2007 to 2012 to 14%. Most of the decline was explained by dietary changes and only small amount (0.14 mmol/l) was explained by increased statin use since the 1980s."