If you look at my second high dose
You will see the effect of an admittedly high dose on the feedback systems for glucose. Because I have long periods between rapamycin I think I see my glucose feedback system stabilising before rapamycin knocks it off balance again. I don’t think it is an immediate thing, but happens after a couple of days and because initially of hepatic insulin resistance and then the other systems over compensate and it ends up with a period of really high insulin responses without the insulin resistance.
I will do another CGM session before I use rapamycin again.
2 Likes
LukeMV
#63
I’ve been doing the same combo of rapa and rosuvastatin and it also raises my A1C. I’m taking a hiatus from Rapamycin for the time being to see if it improves the A1C.
Would an SGLT2 inhibitor take care of this issue in principle?
LukeMV
#65
I use one and it does not take care of the issue.
How is it all supposed to happen then? Mechanistically? I’d think that if glucose is getting dumped out in urine it shouldn’t be available to wreak havoc on internal systems through dysregulation of its oxidization? Or is this a question for ChatGPT deep research mode? Just trying to think of a plausible mechanism.
A_User
#67
It probably decreases absolute amounts of glucose by about 60 g/day, so it’s not going to prevent any increases in blood glucose on top of that.
JeffW
#68
I noticed you’re using Libre. Have you validated the Libre readings with a glucose meter? I found that Libre was consistently off by about 1 mmol/L, so I wouldn’t fully trust the absolute numbers — though the spikes are probably accurate. I’ve since switched to Dexcom, which I find far more accurate, especially since it can be calibrated against a glucose meter.
On a somewhat related note, I started an SGLT2 inhibitor and noticed my A1C rose by 0.4% — despite better glucose control as shown by Dexcom (tight curves, low variability, and 100% time in range). The likely reason? SGLT2s stimulate erythropoietin (EPO), which increases red blood cell lifespan. Since A1C reflects cumulative glucose exposure over the life of a red blood cell, older cells can show more glycation — artificially inflating the A1C, even when actual glucose levels are lower.
2 Likes
snax444
#69
Thanks @CronosTempi , I have edited my post to clarify my points. Basically, i noticed that if I take rosuvastatin 5mg daily, along with sirolimus 5mg weekly, I seem to experience glucose dysregulation. So, as an experiment, I’m trying rosuvastatin 5mg only once a week, to see if it makes any difference to glucose, while also seeing if I still get any significant lipid loweing effect (in addition to Ezetimibe + Bempedoic acid, which I continue to take on a daily basis).
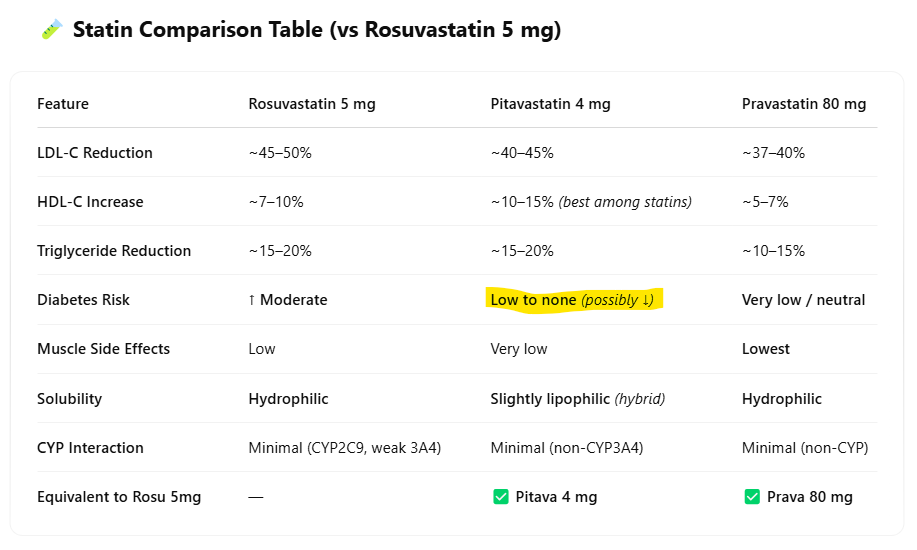
Got it, thank you! Out of curiosity, is there a particular reason you settled on rosuvastatin rather than any other statin? I ask because I myself am prediabetic and trying to lower both ApoB and A1c. And to that end, I switched from 10mg/day atorvastatin to 4mg/day pitavastatin. The idea being that atorvastatin - like rosuvastatin - is linked to glucose disregulation and new onset diabetes, meanwhile pitavastatin is not (also there are many other things to like about pitavastatin).
snax444
#71
Thanks @LukeMV, for sharing your similar experience. You did mention in the past that rosuvastatin alone is not causing glucose dysregulation in your case, so it is more likely rapa doing it (or perhaps in combination)
I will run another experiment taking a 3-month break from sirolimus, will also consider taking a break from rosuvastatin, or perhaps take it less frequently… I’m trying not to change too many variables in my experiment… In my case, I’m not dependent on statins as such, since I believe my risk profile is quite low (CAC score zero, very low Triglycerides 45 mg/dL, very low HomaIR 0.44, hsCRP < 0.4), I’m basically taking low-dose lipid lowering meds to keep my lifetime LDL exposure low.
1 Like
snax444
#72
Noted @CronosTempi. I didn’t have a hard-science reason for picking rosuvastatin as such. Basically, 1) I followed Dr Brad Stanfield’s research videos, 2) took a note that it is water soluble (which I now know may not necessarily be the case, as it could potentially cross the blood brain barrier in some people), and 3) thought that I can get away with a baby dose of 5mg, 4) More potent than other statins, at low dose.
Sure, at some stage, I’ll experiment with other forms of statins (Pravastatin / Pitavastatin) that have some meta-analysis suggesting lowest risk for new onset diabetes.
2 Likes
snax444
#73
Thanks @JeffW , excellent analysis. Yeah, I did think about this one, I understand that HbA1c is not a perfect marker by any means. My Homa-IR is very low at 0.44 when last tested (likely suggesting that my glucose regulation is generally quite good). However, with a combo of weekly rapa + daily rosuva (consistently taken for 4 weeks), I noticed my HbA1c significantly went up (with all other variables largely remaining the same), which prompted me to slap on my CGM (yes, it is Abbott Freestyle Libre 2) to observe the patterns. Sure, will consider using Dexcom at some stage.
snax444
#74
@CronosTempi , here is ChatGPT comparison for equilavent of rosuva 5mg (just for general reference, to be viewed with caution)… At low dose 4mg, Pitava seems to make a good case for me to try
4 Likes
snax444
#75
Interesting viewpoint that does resonate with me
I don’t really see the issue here, to be honest? Your glucose went up after eating a burrito, which isn’t a surprise. And it never went hyperglycaemic. The movement up and down is quite normal because digesting the food over several hours and it’s being constantly absorbed, and you are also clearing it from the blood. If you add activity like walking, that’s going to accelerate the clearance. That is balanced with increasing and decreasing your hepatic glucose output, all aimed at keeping your blood glucose relatively stable. To me, that “up and down” looks like homeostasis working perfectly.
Pretty ambitious, depending on your genetics. Based on the goals, why not add some fasting, taking the Rapamycin at the start of the fast? I think that would give you better mTORC1 activity reduction, and it’s also a way of lowering glucose area under the curve.
1 Like
Matt Kaeberlein reacts to the Chris Masterjohn piece.
Rapamycin: The Worst Longevity Idea Ever Conceived?
13 Likes
PDF of transcript
mk masterjohn.pdf (131.4 KB)
6 Likes
jnorm
#79
“If it’s drilling a hole in your mouth, what do you think it’s doing to your brain?”
Matt’s reaction to the D.A.R.E-level reasoning was priceless.
2 Likes
LukeMV
#80
Another good video with Kaeberlein on Siim Land’s podcast. I like these collaborations.
4 Likes