I would even venture to say he’s “jacked” 
1 Like
Not sure I would necessarily presume rapamycin inhibits muscle growth (even if that seems mechanistically plausible). Completely speculating here but I’m guessing Brad Stanfield’s study will suggest the opposite
1 Like
I agree, caution is advised, biology tends to keep surprising. Brad’s study - it’ll be interesting to see the protocol.
1 Like
He was pretty muscular before. Remember when he did his DEXA? I think his percentile was already 90+ and he was in the low teens for bodyfat.
1 Like
I don’t know, I guess we’re all speculating but to me that falls into the wishful thinking bucket. I hope we learn something from Brad’s study but I don’t know how applicable it will be outside of the elderly population. I don’t know if they’re trained or untrained. If untrained, that would make it even less relevant. I’d like to see a study on 30-50 year old very well-trained men without appreciable anabolic resistance who have healthy muscles (not laced with fat) and are metabolically healthy. Have somebody who knows what they’re doing execute the study: Brad Schoenfeld. Maybe Brad Stanfield will show that rapamycin repairs a broken process in elderly people that then allows them to start putting on muscle again, but that’s a special population and he’s starting from a suboptimal state. I think we’ll learn very little.
My argument as a younger person is that if it reduces my ability to progress my workload, or actually causes it to regress early in the week after dosing, and I’m very confident that it does this, it is inhibiting muscle growth because I’m not giving my muscles the same stimulus that I could get without it. Progressive overload is slowed, and therefor muscle is accruing at a lesser rate. I concede that the effect may be small if we time the dose well, but to say there’s no impact seems like a real stretch. And if I have to adjust my training to avoid mTOR inhibition, it is slowing muscle growth relative to what would otherwise be possible. That’s not mechanistic, but the end result is the same in the real world where it matters - I don’t live in a petri dish. 
But regarding mechanisms, how do we get around this study? Yes, they’re talking about substantial doses and brief windows, but we can’t deny that the impact on MPS is real. Anyway, I’ve made my case. There’s not anything else to add. I actually have to go do leg day right now.
Rapamycin is inhibiting my muscle growth by causing me to spend time debating it on the internet with strangers rather than do leg day.
Rapamycin administration in humans blocks the contraction-induced increase in skeletal muscle protein synthesis - PMC>
The novel findings from this study are the following: (1) the increase in human muscle protein synthesis during the early (1–2 h) post-exercise recovery period is abolished by rapamycin administration prior to exercise; (2) the exercise-induced change in the phosphorylation of a majority of proteins in the mTORC1 signalling pathway (i.e. mTOR, S6K1, rpS6) were delayed with rapamycin treatment; and (3) rapamycin completely blocked S6K1 (Thr421/Ser424), eEF2 (Thr56), ERK1/2 (Thr202/Tyr204), and blunted MNK1 (Thr197/202) phosphorylation during post-exercise recovery.
7 Likes
Agetron
#108
You wrote: “Maybe Brad Stanfield will show that rapamycin repairs a broken process in elderly people that then allows them to start putting on muscle again, but that’s a special population and he’s starting from a suboptimal state. I think we’ll learn very little.” Exactly!
Kind of like the PEARL study - great idea, but when they start off with inferior product rapamycin - Wha - Wha -Whaaa!! https://www.youtube.com/watch?v=lAiI_Vbt5V8
2 Likes
cl-user
#109
@AgentSmith FYI, here is what I get when I run my rapamycin PK model on your values:
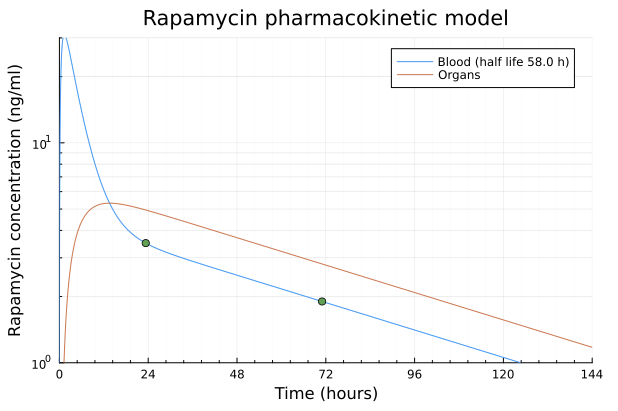
Basically it finds a slightly higher half-life than you because the first point at 23.33h is still a little bit before the equilibrium. That’s why I prefer taking the first point at 48h just to be sure.
This is similar to what I’ve observed myself and I have been using a training schedule similar to yours but then recently, I’ve been thinking that it leave too little time for training in the remaining of the week.
This is why I’ve now started to use a 4 week rapamycin cycle like so:
- Week 1 - No Rapamycin: Training normally
- Week 2 - 6 mg Rapamycin: 3 Day pause then training normally
- Week 3 - No Rapamycin: Training normally
- Week 4 - 12 mg Rapamycin: 5 Day pause then training normally. That’s assimilation/recovery week
Another way to see it is
- 6 mg Rapamycin: 3 days low activity
- 11 days of normal training
- 12 mg Rapamycin, 5 days low activity, 2 days moderate activity (assimilation/recovery week)
- 7 days of normal training
That forces me to plan the training to be sequences of 11 days and 9 days between the rapa intakes but I kind of like it in fact.
I can also adjust it by skipping the 6 mg intermediate dose if I want to train more or bumping it up to 12 mg if I want to train less.
3 Likes
Thanks for running my numbers through your more sophisticated model. I’ll adjust the test timing next time.
I like your training and dosing plan. What kind of results are you getting?
They should have asked the community for feedback first, just as Brad should have. But doctors know better than the rest of us… 
3 Likes
Agetron
#112
Hahaha… exactly… working in isolation isn’t a good model.
Getting feedback helps prevent failures.
2 Likes
Tim
#113
What if rapamycin caused a muscle-wasting disease among the Rapa Nui?
Even if rapa inhibits growth for a few days after your weekly dose, I think that continuing to work out helps with loss prevention.
1 Like
This is all very insightful, and I did read it all the way to the end!
I do wonder if for most people this is similar to Vitamin C + E’s “blunting” effects on training where it was found that the molecular markers are indeed blunted, however the outcome metrics we actually care about were hardly, if at all, effected (strength, endurance, etc). I think the fact that you could perceive a real difference in training is more important than the mechanistic rationale, and I would probably suggest that for most people, they should see what their training looks like without rapamycin and with and focus more on perceived differences than try to create a mechanistically perfect training regimen. I suspect for most people here, myself included, we don’t have enough anabolic resistance to truly see a difference in hypertrophy with weekly rapamycin dosing, especially if one doesn’t notice a difference in perceived output.
4 Likes
cl-user
#115
I’m just starting my training plan for a marathon (3h35 target time) in November so we’ll see how it goes.
2 Likes
Right, probably most here are still too young to worry about anabolic resistance, and that’s easy enough to discern by tracking progress. The question I still have is whether, at least for me, a weekly dose that doesn’t interfere with training is a high enough dose to be worthwhile in the first place. 5 mg seemed to be that dose, yet that’s half of what may be ideal for longevity/healthspan.
Let me reword that slightly. I’ve observed over the past couple years that most on the forum (not all) have said rapamycin doesn’t interfere with their training. Therefore, I have wondered if most are simply not taking enough or just not training super hard (aggressively towards an objective), or both.
One of the questions I asked myself was whether a professional athlete would continue the drug if they noticed the same effect. I assumed not, definitely not, regardless of mechanisms and serum levels. That’s the relevant question during those times when a specific performance goal is my priority. It is not, however, the most relevant question for those prioritizing longevity. I can be either person at different times.
I think I simply want assurance that whatever effort I put into some enterprise is going to have a high probability of producing a significant effect. That means if I’m taking rapamycin, I want to take a hefty dose and I’m not going to try to improve athletic performance or build muscle. And if I’m trying to build muscle or hit a PR, I’m not going to suppress anabolism. But that’s just my personality coming through. I sincerely appreciate all the different approaches and objectives across the community.
3 Likes
A_User
#117
Transforming into his Chad longevity physique. Sarcopenia banished forever.
1 Like
If both strength training and cardio are priorities you could consider cycling what you focus on every week and take rapamycin before the cardio week. For instance this is my plan (completely aspirational - I usually end up doing about half of this at most):
WEEK A – STRENGTH FOCUSED
Mon – Full Body
Tue – Zone 2
Wed – Full Body
Thu – HIIT (Norwegian 4x4)
Fri – Upper/arms
WEEK B – CARDIO FOCUSED
Mon – HIIT
Tue – Zone 2
Wed – Full Body
Thu – HIIT
Fri – Zone 2
That’s not much strength training then. Maintenance at best.
1 Like
Yes - maintenance is the goal during cardio weeks (more than enough strength training to grow during strength weeks)
I don’t think there is any need to worry about exercise adaptation too much. Even if we find out there is a small reduction, you will get most benefits. Having 3/4 tank of gas isn’t as good as having a full tank, but it’s better than being empty.
I think the simplest approach is to do circuit training. That is what I do twice a week (32 minutes times 2), and four times aerobic (jogging with elements of HIIT). Circuit training will not be optimal for muscle hypertrophy, but you can still make gains while not giving up cardio. YMMV.
