GregE
#225
Since increasing my dose to 3-4mg/week with GFJ my PSA has dropped from 6 to 2.6 (4/23) and 2.1 (6/22) with a non aggressive adenocarcinoma (Gleason 6).
It’s likely Dr. B had cancer before '91 and clearly smoked for several decades…as have I! I’m hopeful that my R will buy me time, but not a cure… that would be a fantasy to hope for but not plan on.
8 Likes
Goran
#226
If you have a lot of cancer in your family, you might want to investigate the power of IP-6 Inositol. There is a lot of good reviews on this, and it is very helpful for hormone balance and blood sugar on top of cancer prevention and cancer treatment. It is one of the cheapest supplements out there with no or very little side effects.
After I started taking it, my swollen prostate does not bother me any more, and I sleep like a baby at night. My favorite supplement by far.
9 Likes
LaraPo
#227
I have been taking it for some time. Didn’t notice any side effects. Do you have any?
Thank you. I thought I saw DO (Doctor of Osteopathic Medicine) in Goldhamer’s credentials, not DC.
That does not change the facts they recount, however. Of course, as the patient’s primary physician opined, it could be spontaneous remission.
1 Like
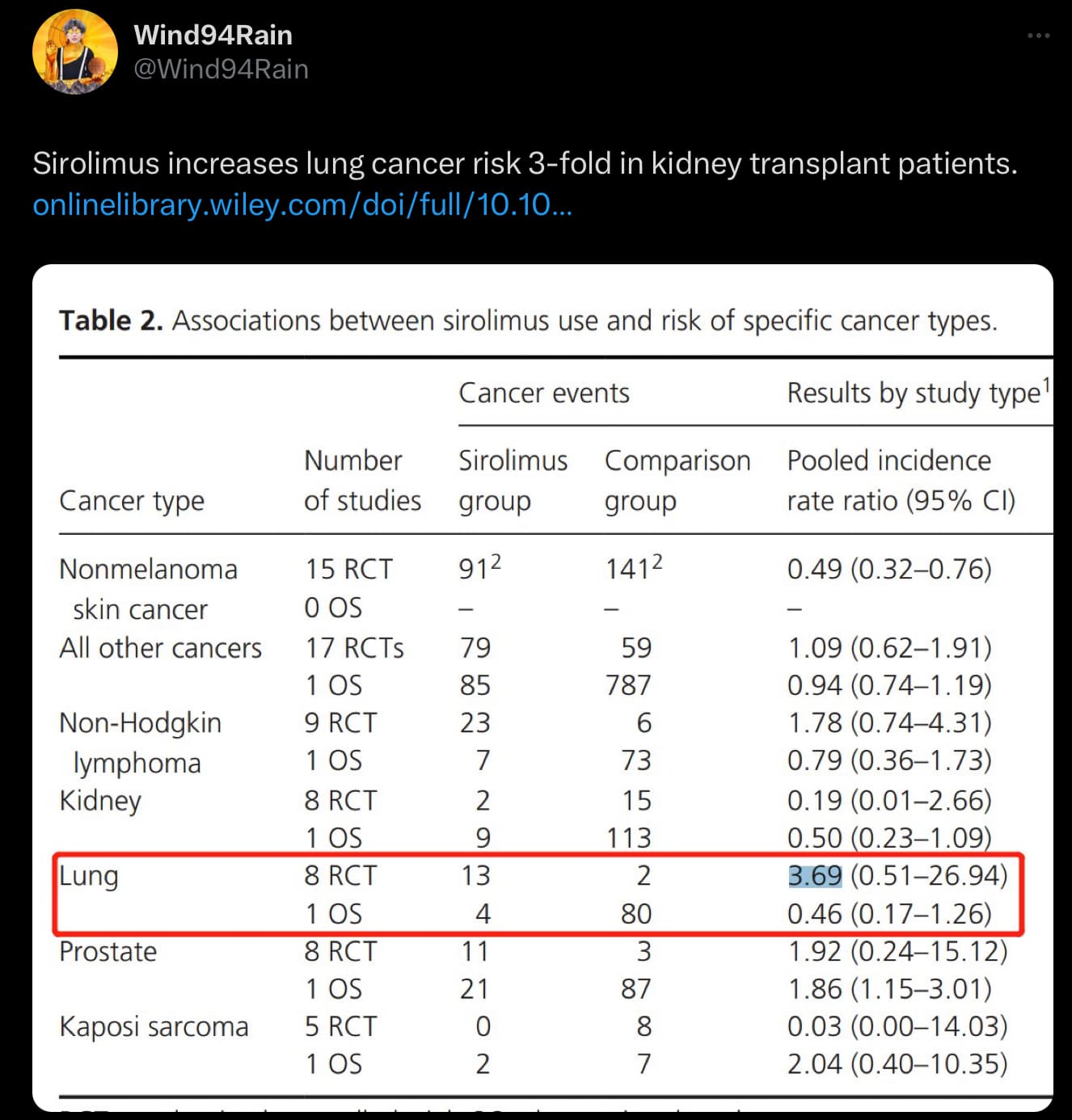
https://onlinelibrary.wiley.com/doi/10.1002/cam4.487
People who don’t understand basic concepts like ‘statistical significance’ or how ‘confidence intervals’ work should not be making public statements about any research. As this contributes nothing but misinformation.
None of these results are statistically significant. Meaning there is a high likelihood that these numbers are the results of pure chance. The only statistically significant result in this photo is the non-melanoma skin cancer.
When the confidence interval ranges from below 1 to above 1, Means the result is not statistically significant.
13 Likes
A_User
#230
Interesting.
The p-value was cropped out which is p-value = 0.780 for lung cancer.
Guess if someone says something like that twitter again, can’t really trust it…
So now we had a very long useless discussion based on an useless study, great.
I feel mislead.
6 Likes
Right. Good point. But it shows that rapamycin is only protective against the most benign skin cancers with any clinical significance or confidence level.
Blagosklonny has correctly made the point on many occasions that we don’t die of aging, we die from aging- related diseases. So we’re talking primarily about CAD, AD, and cancer.
Do we have evidence in humans that it’s preventing these diseases? Or do we just have mice which translates poorly to us?
Are we walking a fine line since we have virtually no idea how to dose it?
Would we, as doctors, ever prescribe a drug based solely on mice?
I’m not saying to stop the drug. But we shouldn’t be fooling ourselves either.
9 Likes
@Dr_Rami_Abunadar Thanks for pointing this out. You are correct in your assessment.
For me, I will continue to take Rapamycin. It’s not just one mouse study, but 64+ studies on every model organism that responds well to Rapamycin.
The Dog Aging project has had several positive anecdotes, and that’s one step up on the food chain. Hopefully, we will have more information from this study soon to help us make decisions.
The correct dosing is the most pressing issue here. We just don’t have enough data to make a great choice. A very high dose could be good or bad. However, a moderate dose (3-6 mg weekly) seems to be what the experts have chosen and seems to be well tolerated.
Let’s hope for some more clarity on this issue… or for something better than Rapamycin to come along…
5 Likes
That table is such a poor way to present data as you’ve said. Look also at the prostate cancer incidence for observational studies. The 1.86 (1.15 - 3.01 95% CI) also doesn’t cross 1, so is statistically significant. You can see numerically there are more cancers in the observation groups than in rapa, but the 1.86 indicates an 86% higher rate for rapa. At least it should if the table were being consistent in its reporting. To illustrate this inconsistency, the rate for nonmelanoma skin cancer is stated as 0.49, indicating a 51% decrease in the rapa group.
When rapa is better, the rates should be less than 1. When rapa is worse, the rates should be greater than one. Based on the prostate cancer rate of 1.86, I’d bet they flipped the numbers of cancer in each group and it should be 87 in the rapa group and 21 in the comparator. That would also be more consistent with the numbers reported in the RCTs for prostate cancer
1 Like
@Goran and @LaraPo which IP6 are you using? At what dose?
1 Like
Goran
#236
I take the one from Jarrows formula.
3 Likes
@Goran What dose IP 6-Inositol did you use for your prostate?
I don’t think he would try to do that. This is what he just said in Twitter: Valter Longo sells junk food (really junk) and call it “fasting”  ]. Fasting costs zero and is much more effective. Someone may sell one egg for huge price (on condition that the buyer will not eat anything else), it would be much better. Or egg + a nut, or whatever
]. Fasting costs zero and is much more effective. Someone may sell one egg for huge price (on condition that the buyer will not eat anything else), it would be much better. Or egg + a nut, or whatever
José
#239
scta123
Just to add to you posting/question
Review the published work by Prof AbulKalsm Shamsuddin, MD, PhD
He is the person who created the IP6 compound. Also started/involved in a company that manufactures the compound{IP6] If I recall he has a patent on this.
Member “rivasp12” is the person who mentioned this compound to me on this forum over a year ago.
“rivasp12” knows him personally.
A general knowledge book titled;
“IP6 + INOSITOL”
Was written by Dr. Shamsuddin.
I do not have any financial interest in this book link.
4 Likes
Goran
#240
500mg in the morning and 500mg before I go to bed
2 Likes
LaraPo
#241
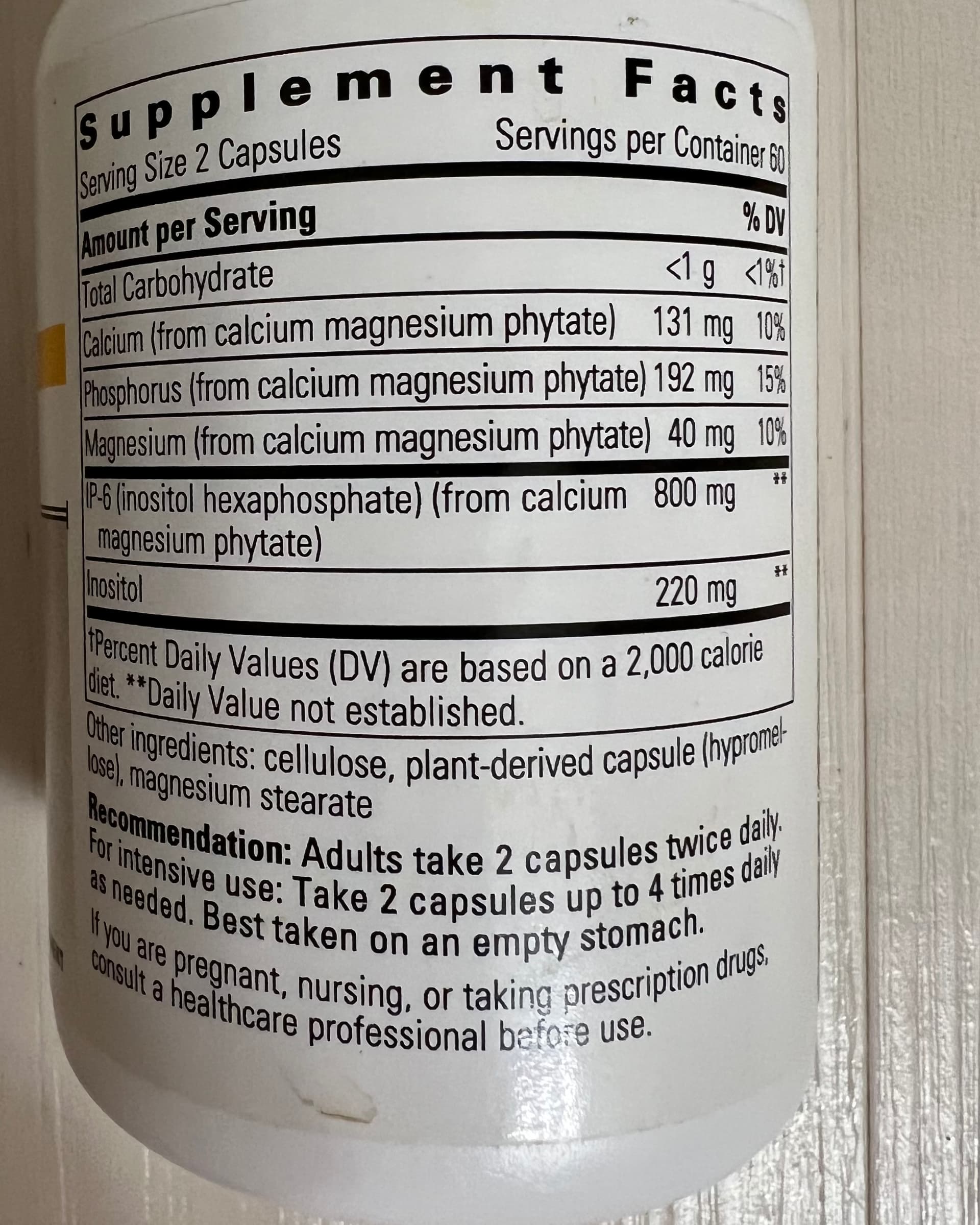
Mine is Integrative Therapeutics, Cellular Forte
3 Likes
I think most if not all of the IP6 is made by a Japanese company (I can’t remember the name of the company). The late Bill Sardi, who I was friendly with was meeting with this company when they came to Las Vegas for the Supply Side West show. I know this went on for at least a couple of years. Bill was a formulator and almost certainly had an idea for a new product, most likely IP6 related. I wish I had asked him what he wanted from them. His death was unexpected.
1 Like
José
#243
FWIW
About Prof AbulKalsm Shamsuddin, MD, PhD
The company he is affiliated/founder;
http://ip-6.net
GregE
#244
Kidney transplant patients that ‘take’ Rapamycin also take other immune suppressive meds along with Rapamycin. Daily Rapamycin builds intentionally to levels toxic to mTOR2 the immune systems. Cyclosporin and other immune suppressive drugs also open the door to cancer.
Never judge a drug at a dose that has a radically different application.
I take weekly Rapamycin, 12mg/week. I do not take immune suppressive medications. I have cancer.
4 Likes
LaraPo
#245
Did you have cancer before you started taking Rapamycin?
1 Like