New email from Brad Stanfield…
Debunking the High Protein Diet Panic
Recently, a headline from the New York Post caused quite a stir: “You might be eating an artery-damaging amount of protein, new study warns.”
This statement, based on a study in Nature Metabolism, set off alarms across social media platforms, including among my YouTube channel viewers, where I’ve shared my adherence to a high-protein diet.
Let’s dissect the facts to understand the real implications of this study.
The research began by referencing animal studies that associate high-protein diets with atherosclerosis development, potentially due to the overstimulation of a specific enzyme known as mTORC1.
The authors posited a human protein intake threshold that might trigger mTORC1 overactivation, leading to heart disease.
Their investigation unfolded across two experiments:
- Liquid Meal Test with 14 Participants: This test compared the effects of a 10% protein meal versus a 50% protein meal after an overnight fast.
- Real-Food Scenario Study: Mimicking everyday meals, this study used liquified real foods, contrasting a standard 15% protein meal against a high-protein meal containing 22%.
The findings confirmed that high-protein diets do indeed activate mTORC1, aligning with initial hypotheses, whereas lower protein intakes did not. They pinpointed that dietary protein intakes exceeding roughly 25g per meal (or ≥22% of energy requirement) activate mTOR signalling in monocytes/macrophages.
From these observations, the authors concluded that:
- mTORC1 overactivation in mice is linked to vascular blockages.
- High-protein meals activate mTORC1.
- Thus, high-protein diets may cause vascular blockages.
Why These Conclusions Are Misleading
The narrative spun by the study and subsequently by the media is misleading for several reasons.
We possess substantial real-world evidence contradicting the notion that high-protein diets harm cardiovascular health.
For instance, a 2023 meta-analysis encompassing 6 studies with 221,583 participants found no association between high-protein diets, cardiovascular disease, or strokes. Moreover, a 2020 BMJ meta-analysis indicated that higher protein intakes correlate with reduced all-cause mortality rates.
This existing, robust data overshadows the new study’s reliance on animal models and biomarkers for its conclusions.
In light of this, here’s my guidance to my patients:
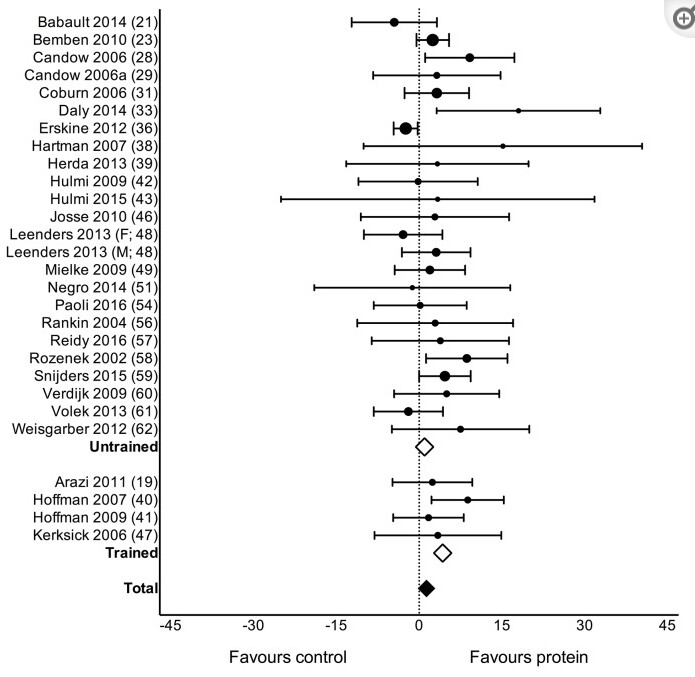
- Engage in resistance training.
- Amplify the benefits of your workouts with a high-protein diet, targeting 1.6 grams per kg of body weight.
- View the new study with skepticism—it’s more sensationalism than science.