I finished the listening today. Fascinating interview. Dr. Fahy is very eloquent and convincing but I wonder, as Kaberlein wondered, why investors are not so interested in his trials.
Towards the end they discuss IGF-1. Strangely, I wasn’t aware that the purpose of the GH administration is to elevate the levels of IGF-1, which apparently causes thymus rejuvenation.
I’ll have to search and see the IGF-1 in the trial participants before and after, if published.
Also, Matt asked about the prevailing models of IGF-1 optimization in the longevity narrative.
Model 1: high IGF-1 is bad because it may cause cancer proliferation. The model supported mainly by the vegan community, but also by eminent gerontologists like Longo and Fontana.
Model 2: IGF-1 is good because it stimulates the immune system, by means, in the hypothesis of Dr. Fahy, of reversing thymus degradation.
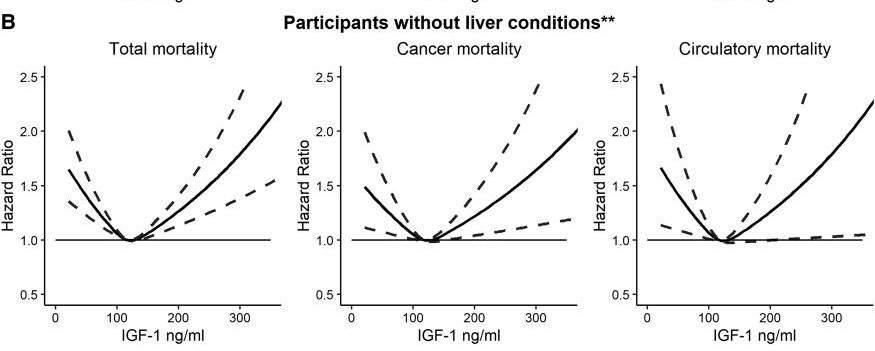
I wonder who’s right. Probabaly both, since there is a U-curve relationship with an optimum, meaning that too little of it may affect detrimentally the immune system, too much of it may provide cancer cells with a potent proliferation signal.
In my own situation, I can objectively observe that I have no problems so far with the immune system, which appears to be well regulated. In the last 10 years, I got a fever once a year on average, with 2 days on average per year desiring to be in bed, sleep, and do nothing else. That is not superhuman immunity but I find it satisfactory.
The alternative is to seek elevated IGF-1 but be on the lookout for precocious cancer formation, which can be very tricky. Also, I erroneously believed that GH can alleviate joint pains, but it seems that it is the opposite.