Really good question!
2 points, in the comparison of DPP-4-i vs GLP’s health outcomes seem significantly worse with DPP-4’s, which may represent that the GLPs are just such awesome drugs that they provide a multiple of the benefit, or it could be that the DPP-4’s are deleterious. The problem with the study with looking at Alzheimer’s Dementia was no control group. However, there are multiple studies indicating that DPP-4’s are beneficial for neurocognitive decline, but the mechanism is likely through increasing GLP/GIP endogenously. I’m not sure if the addition of DPP-4s to GLPs helps if getting an adequate dose of GLP/GIP medication like Tirzepatide?
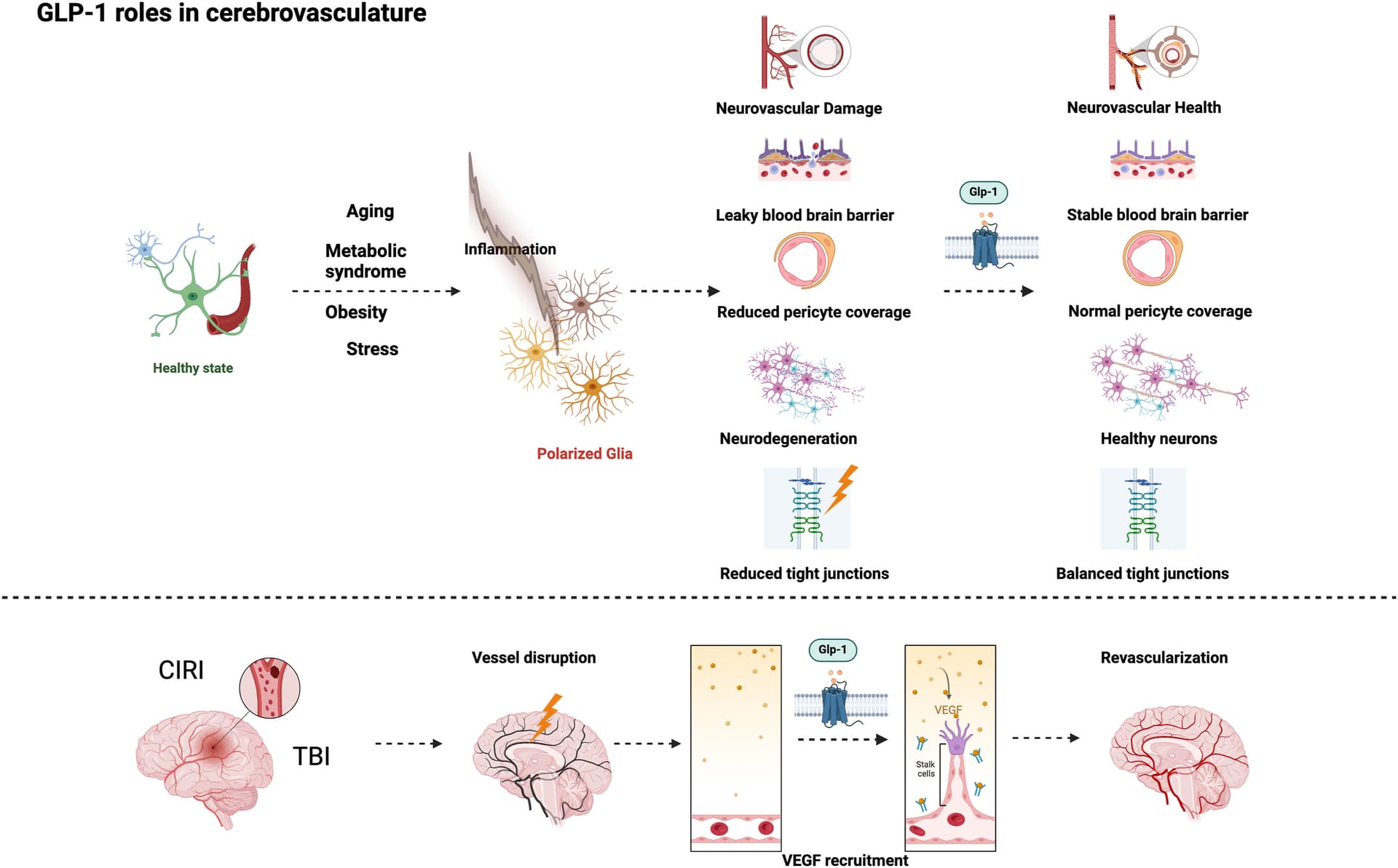
I was thinking if the DPP-4i’s ended up crossing the BBB it could be a good way to increase GLP activity in the brain. Sadly, they don’t significantly cross the BBB.
So Vera-Health.ai does a good job answering this question - and my conclusion is that I generally don’t see a reason to Rx these meds except as a 4th agent for difficult to control T2DM.
Dipeptidyl peptidase-4 (DPP-4) inhibitors do not directly prolong the half-life or increase the effect of GLP-1 receptor agonists (GLP-1 RAs). Instead, they work by inhibiting the DPP-4 enzyme, which is responsible for degrading endogenous GLP-1 and GIP (glucose-dependent insulinotropic polypeptide). This inhibition results in increased levels of endogenous GLP-1 by preventing its breakdown, leading to a modest increase in GLP-1 levels, typically 2-3 times the baseline 6.
GLP-1 RAs, such as exenatide and liraglutide, are synthetic analogs of GLP-1 that are designed to resist degradation by DPP-4, thus having an inherently longer half-life. These drugs are engineered to have prolonged action independently of DPP-4 activity, which means their pharmacokinetics and pharmacodynamics are not significantly altered by concurrent DPP-4 inhibitor use 2.
While DPP-4 inhibitors enhance the duration of action of endogenous GLP-1, they do not directly increase the pharmacological effect of GLP-1 RAs. The complementary mechanism of action between DPP-4 inhibitors and GLP-1 RAs can enhance the overall incretin effect, but this does not translate into a direct prolongation of the half-life or increased effect of GLP-1 RAs themselves 8.
In clinical practice, the combination of DPP-4 inhibitors and GLP-1 RAs is generally not recommended due to overlapping mechanisms and limited additional benefit. Most guidelines suggest using either a DPP-4 inhibitor or a GLP-1 RA, but not both simultaneously, to manage type 2 diabetes mellitus (T2DM) 1.
In summary, DPP-4 inhibitors extend the half-life of naturally occurring GLP-1 by blocking its degradation, thereby sustaining its beneficial effects on glucose regulation. They do not directly increase the pharmacological effect of GLP-1 drugs, which are already designed to have prolonged action independently of DPP-4 activity. This distinction is crucial for understanding the complementary roles of DPP-4 inhibitors and GLP-1 receptor agonists in the management of T2DM.