Beth
#123
Edited my question because I see HS crp vs CRP doesn’t change the value much… I’m either 12-14 years younger… I’ll take either!
1 Like
The molecule is the same. HS (High Sensitivity) refers to the test.
2 Likes
blsm
#125
This is a smallish update-
My gluten challenge took longer than I planned due to vacation limiting my access to the particular bread I was eating. I didn’t end up making it the full 14 days. Everything was seemingly going well until day 11 when my body obviously had enough! Hahaha, I’ll spare you all the details! 
In the past I would get dermatitis herpetiformis outbreaks/reactions within a day or two of any trace gluten exposure and in this experiment of 2 slices of bread per day it only obviously impacted my gut. I’m happy I tried though and pleased my body isn’t nearly as sensitive.
I’m continuing to eat a no added salt diet which is working out great for me personally. I do regret my years of excessive salt consumption and think it caused a lot of issues I (not any of my doctors) could never quite put my finger on starting in my teens. Here are my personal improvements:
*I stay hydrated pretty effortlessly
*No longer have dizzy spells, weakness, fatigue if I push myself too hard
*BP is in a rock solid stable range of 90-100/60-70. (Systolic goes up to 115 temporarily with exercise)
*I never have facial puffiness
*My skin no longer feels tight/dry without lotion
Here’s a screenshot of my dietary sodium to potassium ratio intake for the week.
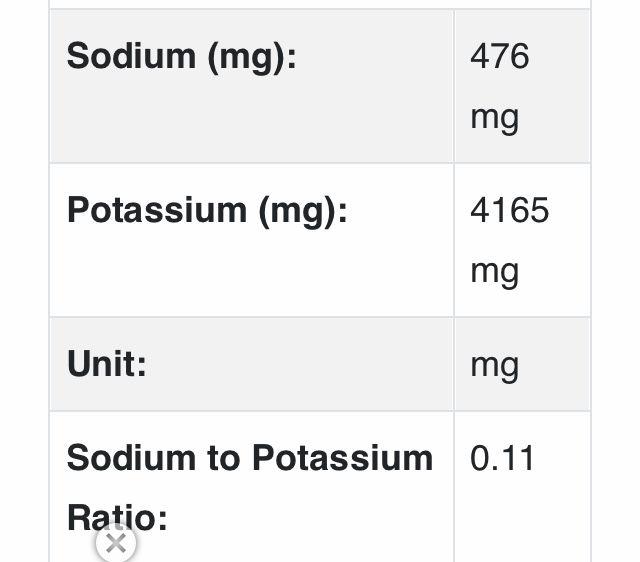
I’m slightly higher than the Yanomami but it’s not bad for living in the modern world!
I’m going to try to run more labs by the end of September. I’m hopeful for continued improvements since I’m now able to tolerate a more plant based diet with some fish/shellfish. I still have some lean meat, eggs and non fat dairy about 50% of the time but it’s a far cry from the 100% carnivore diet I was eating when I joined. I’m grateful for the education I’ve received here from so many members that inspired me to be persistent in breaking away from a dietary pattern that really wasn’t working for me.
2 Likes
Are those the daily figures averaged for the week or the week’s figures?
1 Like
blsm
#127
I plugged my average intake from cronometer for the last seven days into the calculator. Hopefully I’ve understood your question correctly but let me know if not please!
blsm
#128
5 Likes
blsm
#129
I’ve decided to take the plunge with Ageless for my rapamycin. I’ve been taking Biocon/Eris Rapacan since January of 2023 with good results but with the current import situation I had to figure out an alternate plan. My labs were just drawn so hopefully later this week if everything looks satisfactory the medication will be shipped.
I’ll share my labs when the results are in. I’m actually pretty excited to start having my sirolimus levels monitored and have some professional oversight.
3 Likes
blsm
#130
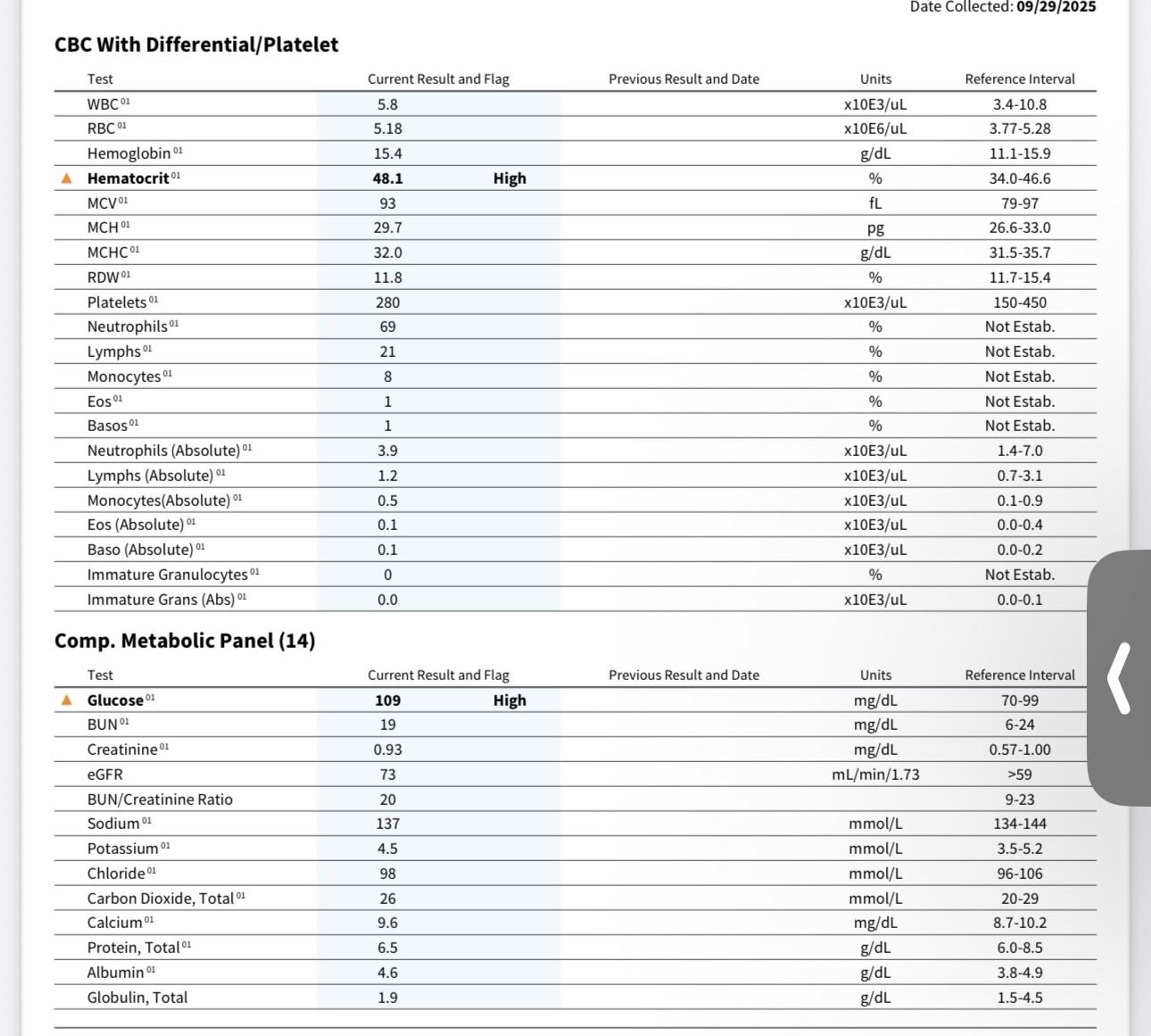
Here’s my meh labs from ageless. I’m going to start a statin very soon.
My ldl is still a bit too high at 72 mg/dl. I’ve been taking a 5mg dose of ezetimibe for close to six months and I believe it probably does next nothing for me tbh.
My fasting glucose was oddly high at 108 mg/dl so I’m going to recheck it myself. I’m actually having a hard time believing it’s reflective of my norm. I’ve been on dapagliflozin (5mg) for close to six months. I’ve also been eating in a surplus in an effort to put on a little weight and although I’ve succeeded that could have impacted my numbers. I was concerned about that happening. Beyond that I think I might have been coming down with a cold that I caught from my husband and didn’t know it yet on the day I got my blood drawn. I’ve read sickness can impact glucose. I also took an extended release melatonin before bed fwiw. I know that all sounds like a lot of coping! Hahaha
My eGFR is worse as well which I need to get a handle on and recheck. I had read that could happen with the flozins in the first 6 months so hopefully it normalizes.
It will be interesting to see if ageless will provide me with rapa in light of the labs. If not I got a message from one of my Indian connections at 1am that he’s resuming shipments to the US.
4 Likes
For fun I threw your test results into CGPT5 with the prompt:
Provide an indepth analysis and summary of the attached blood test results and identify measures that are less than optimal, when considering optimal are those levels identified by Peter Attia according to his Medicine 3.0 definition. Identify strategies to get the markers that are out of the optimal range, back into the optimal range. Please identify approaches for each of the measures that need improvement.
Response:
Here’s a full Peter Attia “Medicine 3.0” style interpretation of your recent blood panel, using optimal (not just normal) targets — and specific, evidence-based actions to move each parameter toward Attia’s preferred ranges for long-term health and longevity.
 Overview
Overview
Your overall profile is excellent — strong hematologic, metabolic, and lipid parameters with very low inflammation.
A few readings are borderline elevated or suboptimal from an optimization standpoint (not pathology), particularly:
| Category |
Marker |
Status vs Optimal |
Interpretation |
| Erythrocyte |
Hematocrit 48.1% |
Slightly high |
Possible mild erythrocytosis (testosterone/altitude/dehydration) |
| Glucose control |
Fasting glucose 109 mg/dL |
High (prediabetic range) |
Suggests mild insulin resistance or late postprandial draw |
| Glucose control |
Insulin 6.1 µIU/mL |
Borderline optimal |
Great, but fasting glucose suggests occasional dysregulation |
| Lipids |
HDL 57, LDL 72, TG 59 |
Optimal |
Excellent atherogenic profile |
| Inflammation |
CRP 0.30 mg/L |
Excellent (low) |
Very low inflammation |
| Liver/kidney |
All optimal |
— |
Normal function and detox capacity |
| Sirolimus |
<0.5 ng/mL |
Below target range |
Suggests subtherapeutic trough depending on dosing strategy |
 CBC Interpretation
CBC Interpretation
| Marker |
Your Value |
Optimal Range (Attia/functional) |
Comment & Strategy |
| Hematocrit |
48.1% (High) |
40–46% (men) |
Mildly elevated — common with testosterone, dehydration, or high-protein intake.
Strategies: Hydrate well, check ferritin and EPO levels, consider donating blood every 3–4 months if persistently >49%. Ensure oxygen saturation >95% (sleep apnea raises Hct). |
| Hemoglobin |
15.4 |
13.5–15.5 |
Perfect; consistent with healthy oxygen transport. |
| RBC count |
5.18 |
4.3–5.2 |
Upper-normal; consistent with slightly elevated Hct. |
| WBC |
5.8 |
4.0–6.0 |
Ideal — suggests balanced immune state, no chronic inflammation. |
| Differential |
Normal |
— |
No infection, allergy, or immune imbalance indicated. |
| Platelets |
280 |
180–350 |
Optimal. |
 Metabolic Panel
Metabolic Panel
| Marker |
Your Value |
Optimal (Attia) |
Comment & Strategy |
| Glucose (fasting) |
109 mg/dL (High) |
75–90 mg/dL |
Mildly elevated — can indicate transient insulin resistance or stress/cortisol surge.
Strategies:
• Retest fasting after 12–14 hrs, low-carb dinner prior.
• Reduce evening carbs, optimize sleep (lowers AM cortisol/glucose).
• Add 20–30 min post-meal walks.
• Consider CGM use to check glycemic variability.
• If persistent >100 mg/dL, test fasting insulin, HOMA-IR, and 2-hr OGTT. |
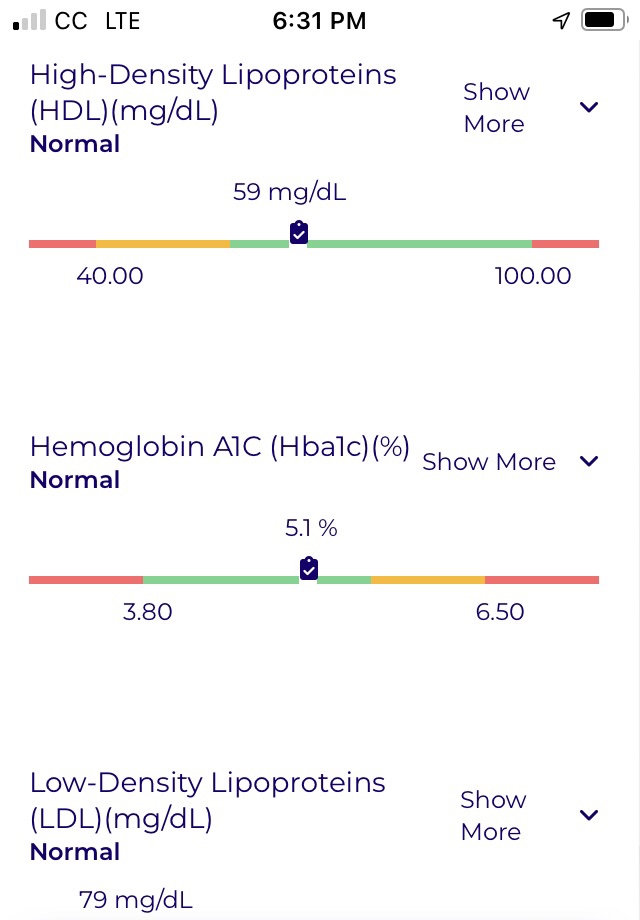
| Hemoglobin A1c |
5.3% |
4.8–5.2% |
Great; near-optimal long-term glycemia. Small improvement possible via reducing postprandial spikes. |
| Insulin (fasting) |
6.1 µIU/mL |
2–5 µIU/mL |
Slightly above Attia’s ideal range — consistent with fasting glucose elevation.
Strategies:
• Maintain low refined-carb diet (under 100g net/day).
• Add strength training or 24–36 hr intermittent fasting once/week. |
| eGFR |
73 mL/min/1.73 m² |
>70 |
Healthy renal function; track trends yearly. |
| BUN / Creatinine |
19 / 0.93 |
Optimal |
Balanced protein metabolism; nothing to adjust. |
| Electrolytes (Na/K/Cl/CO₂) |
Ideal |
— |
Excellent fluid and acid-base balance. |
| Liver enzymes (AST/ALT/ALP) |
20 / 18 / 50 |
<25 / <25 / <100 |
Outstanding liver health; supports rapamycin safety. |
 Lipid & Inflammation Panel
Lipid & Inflammation Panel
| Marker |
Your Value |
Optimal (Medicine 3.0) |
Comment & Strategy |
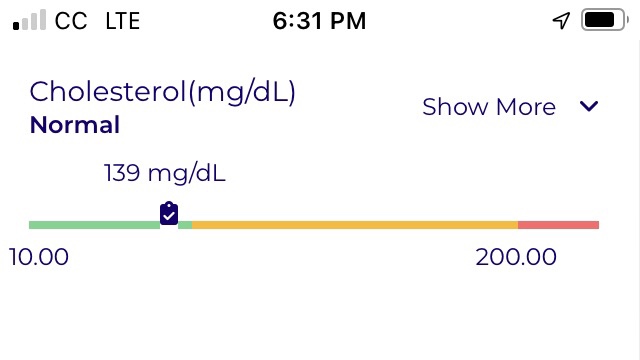
| Total Cholesterol |
141 mg/dL |
<160 |
Very good. |
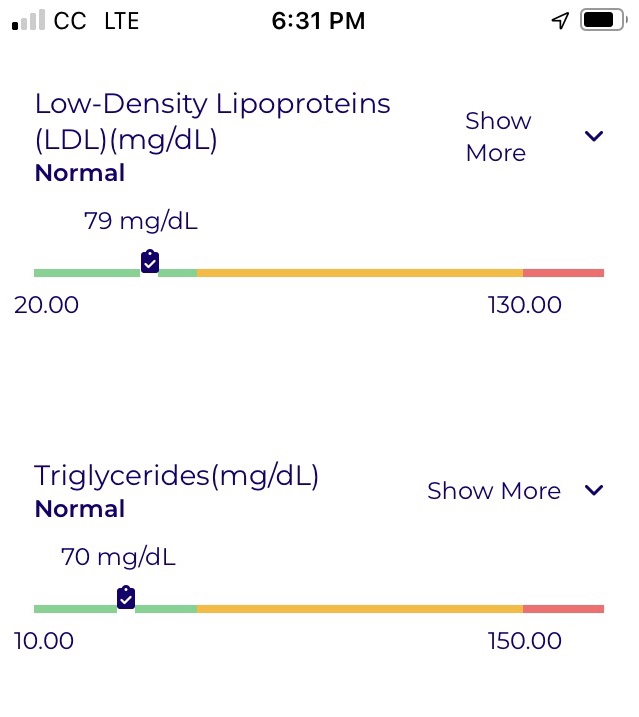
| LDL-C (NIH) |
72 mg/dL |
<70 (Attia optimal) |
Near-optimal. ApoB or LDL-P testing would better define risk. |
| HDL-C |
57 mg/dL |
>50 |
Excellent. |
| Triglycerides |
59 mg/dL |
<70 |
Excellent insulin sensitivity marker. |
| CRP (cardiac) |
0.30 mg/L |
<0.5 |
Superb — very low systemic inflammation. Maintain through omega-3 intake, exercise, oral health. |
 Sirolimus (Rapamycin) Level
Sirolimus (Rapamycin) Level
| Marker |
Your Value |
Target Range (Longevity-use) |
Comment & Strategy |
| Sirolimus trough |
<0.5 ng/mL |
3–6 ng/mL (ITP/longevity dosing analog) |
Below detection — indicates subtherapeutic exposure. If you dosed >5 days before draw, likely cleared.
Strategy: Confirm timing post-dose (24 hr = trough). If intentionally pulsed weekly, target 3–6 ng/mL at 24 hr post-dose, returning to <1 by day 5–6. Adjust dose or timing as desired. |
 Inflammation & Longevity Biomarkers
Inflammation & Longevity Biomarkers
| Marker |
Your Value |
Optimal Range |
Comment |
| CRP |
0.30 |
<0.5 |
Excellent anti-inflammatory status — likely due to good metabolic control and lifestyle. |
| Albumin |
4.6 |
4.2–5.0 |
Excellent; predictive of longevity. |
| Globulin |
1.9 |
2.0–2.5 |
Slightly low but not concerning; maintain via adequate protein intake (≥1.6 g/kg/day). |
 Summary of Focus Areas
Summary of Focus Areas
| Priority |
Marker |
Issue |
Strategy |
 |
Fasting glucose (109) |
Mild insulin resistance or timing artifact |
Recheck fasting; lower late carbs; use CGM; improve sleep and activity timing |
 |
Insulin (6.1) |
Slightly elevated |
Lower glycemic load, increase resistance training, possible metformin if persistently elevated |
|
Hematocrit (48.1%) |
Slightly high |
Hydrate, check ferritin/EPO, donate blood if >49%, check sleep apnea |
 |
Sirolimus <0.5 ng/mL |
Below therapeutic target |
Confirm timing vs dose; adjust schedule if goal is systemic effect |
 |
CRP, LDL, HDL, TG, A1c |
Optimal |
Maintain via exercise, sleep, micronutrients, omega-3s, and fiber (30–40g/day) |
 Lifestyle & Supplement Optimization
Lifestyle & Supplement Optimization
-
Metabolic Control
- Time-restricted eating (10–12 hr eating window).
- Add berberine 500 mg 2×/day or acarbose 25–50 mg before carb meals.
- Regular HIIT and resistance training 3–5×/week.
- Target fasting glucose <90 and mean CGM <100 mg/dL.
-
Erythrocyte Regulation
- Donate blood every 3–4 months if hematocrit >49%.
- Avoid dehydration and ensure good sleep quality (screen for OSA).
-
Rapamycin Optimization
- Measure trough 24 h post-dose.
- Typical weekly dose (for translational equivalence): 5–10 mg oral.
- Consider co-administration with grapefruit juice (CYP3A4 inhibition) only if experienced and monitored.
-
Maintain Anti-Inflammatory State
- Omega-3 index ≥8% (2–3 g/day EPA+DHA).
- Oral health and gum care.
- Low seed-oil, low-refined-carb diet.
3 Likes
blsm
#132
Thank you so much! I do feel a little bit better about everything and after reading the explanations it all makes perfect sense.
1 Like
blsm
#133
It looks like I finally (hopefully) got my lipids optimal. I’m on a half dose of Ezetimibe at 5mg, a very low dose of rosuvastatin at 2.5mg plus I’m eating about 90% vegan at this point.
All input is appreciated of course.
11 Likes
Looks fantastic to me. Great job!
Why only half a dose of Ezetemibe? How much lower would it be on a full dose?
1 Like
blsm
#135
If you were me would you go higher? I was formerly kind of afraid of lipid lowering meds due believing various (incorrect) influencers on the internet. It’s embarrassing to admit this of course but it’s the truth. Hanging around here has cured me of that but it’s why I started low with both meds. I had improved my numbers quite a bit already with diet prior to starting them.
My dilemma is trying to keep weight on while still eating in a way that doesn’t completely wreck my lipids and glucose. My glucose could still use a bit of improvement with a hbA1c of 5.3 and fasting glucose of 89 on 5mg Dapagliflozin.
2 Likes
I’m in the ‘lower lipids as much as possible’ camp, so I take Ezetimibe 10 mg with my BA and 5 mg Atorvastatin. However, my values are a little higher than yours at LDL 64 and ApoB 58. These are a bit higher than I would like, but I don’t want to increase my statin dose as I am intolerant, and I feel a PCSK9I is overkill for me.
2 Likes
A_User
#137
Your eGFR has decreased by nearly 30 points the past few years, check Cystatin C and other kidney markers, and do a urine analysis for kidney health IMO.
Did you start creatine supplement awhile ago which artificially can increase creatinine?
Kidney function decrease over time so having a good function to begin with is important (decrease in kidney function massively increase risk for CVD and other things… and they’re necessary for life obv).
Rapamycin can impact the kidneys by the way. Peter Attia monitors for it.
2 Likes
blsm
#138
Thanks for the input Chris. It seemed like the miniature statin dose is what really moved the needle for me the most. I’m not sure Ezetimibe did much but I’m sure it hasn’t hurt anything. I’ll probably play around with adjusting my dosages a little. I’m thinking I’ll probably go back to eating a bit more animal foods after Christmas as well just for practical purposes so I’m also interested to see how that impacts my numbers.
1 Like
blsm
#139
I had noticed the decline in my eGFR as well. I was hoping it was just temporary from starting dapagliflozin but I’ll do the Cystatin C test. I really like dapagliflozin but it might not be the right med for me. Thanks for pointing this out so I keep it top of mind. Hopefully I didn’t do any permanent damage. There’s also the fact that I’m female and the flozins do not seem resoundingly positive for women.
As far as rapa goes I haven’t been taking it very regularly over last 4 months due to my high pathogen exposure at work and having numerous skin biopsies on areas I ignored for years (not unlike my lipids). It seems I need make some adjustments. Thanks so much your reply.
Edit-I actually stopped taking creatine a couple months ago.
A_User
#140
I skimmed past your reports, I might have the dates wrong:
Feb 2023: eGFR 93
June 2023: eGFR 106
Dec 2023: eGFR 99
May 2024: eGFR 81
Oct 2025: eGFR 73
In July 2023 you said you added 5 g creatine. I would check whatever you’ve done differently between Dec 2023 and May 2024 (here you said you’ve been on 16.5 months of rapamycin). But yeah Cystatin C is good to add. In Oct 2025 you said you’ve been on dapagliflozin for 6 months, but your eGFR declined as well from Dec 2023 and May 2024, that’s before dapagliflozin. Do you check your blood pressure regularly as well?
2 Likes
blsm
#141
A sincere Thank you for pulling together my numbers. Seeing it that way really hits home. My bp is good at @105/65 without meds. I’m also not obese or diabetic but I suppose you can develop kidney problems from other factors. I have also been on a low sodium diet consistently for the last couple years. The fact that going on a no added salt diet helped me so much may point to some underlying kidney insufficiency as well. I’ll definitely take this seriously!
1 Like
blsm
#142
I just checked and my latest eGFR from 11/7/25 was even lower at 67.
I was reflecting further on what was going on in my life around the time of the decline and it coincided with my high protein phase. I suppose it’s possible I had something going on with my kidneys that wasn’t presenting and the higher protein diet made things worse.