It does seem like they messed up that diagram in the rush to get the news out. If it delayed progression of the marker and was more potent in the ApoE carriers, then why is the marker more positive while being lower or even negative in the placebo group?
Maybe it’s supposed to represent “% inhibition of progression”? This, more positive and higher is better.
1 Like
I think they screwed up the legend in the version you posted. What interests me here is that, on placebo, there is a clear pattern where one e4 makes p-Tau 217 accumulate faster than no e4, and homozygous e4 accumulates even faster. What’s interesting is that the impact of Obi is strong enough to regress p-Tau 217 accumulation in homozygous e4 but only slows accumulation in the others.
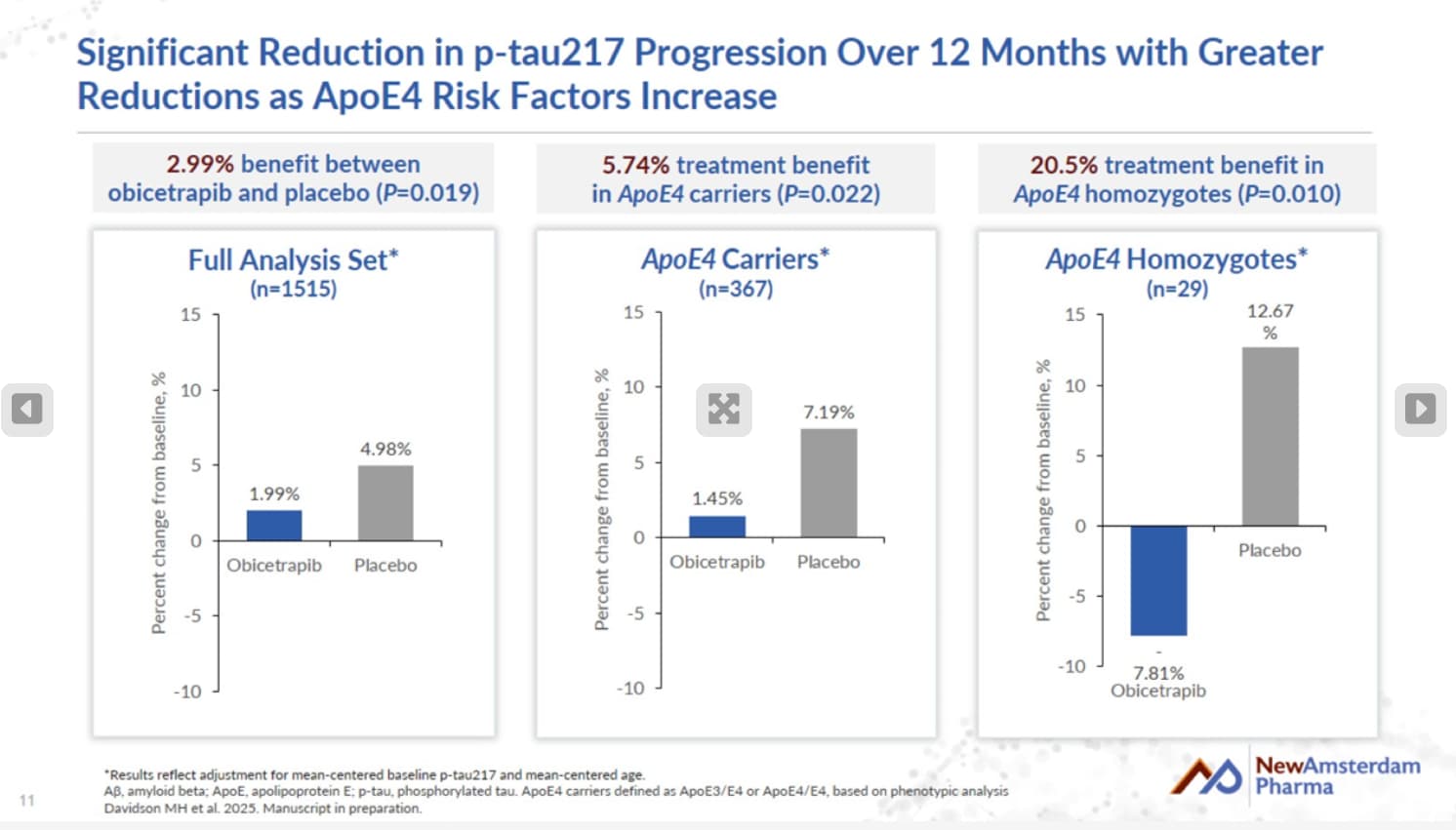
The ‘All prticipants’ graph shows that those on obi saw a 1.99% increase in p-Tau217 levels, whereas the placebo group saw a 4.98% increase. Hence a 2.99% reduction for obi vs. placebo
The ApoE4 subset saw a 1.45% increase on obi vs. 7.19% increase for E4’s on placebo. Hence 5.74% reduction.
E4/E4 saw a 7.81% DECREASE vs. 12.67% increase for E4/E4’s on placebo. Hence 20.48% reduction.
https://ir.newamsterdampharma.com/events/event-details/newamsterdam-conference-call-aaic-2025
4 Likes
Ergo the legend was reversed as suspected. Interesting that E4/E4 is worst case untreated but best response treated.
Assuming equal randomization to placebo and obi in both the whole study population and the ε4 carriers, that would be roughly 2.16% vs. 4.27% increase in the noncarriers. Not shabby, though it would have been nice to see even a slight a decrease like in the ε4 homozygotes.
adssx
#166
Reminder: in MR, CETPi seems useless for AD (but beneficial for LBD and PDD): Obicetrapib (CETP inhibitor for dyslipidemia) - #135 by adssx
2 Likes
adssx
#167
Obicetrapib significantly increases plasma and high-density lipoprotein (HDL) levels of lipophilic antioxidants 2025
Results: Obicetrapib 10 mg/day increased HDL by 159%. In the HDL fraction, obicetrapib 2.5mg significantly increased all antioxidants at V3 with lutein and α-tocopherol increases (48.44% and 48.50%) maintained at V5. Obicetrapib 5mg significantly increased lutein, zeaxanthin, β-cryptoxanthin, γ-tocopherol, and α-tocopherol at V3, by 25.02%, 35.03%, 99.08%, 49.15% and 47.94%, with more marked increases at V5. Obicetrapib 10mg significantly increased lutein, zeaxanthin, β-cryptoxanthin, β-carotene, γ-tocopherol and α-tocopherol at V3, by 38.16%, 37.43%, 109.67%, 86.99%, 42.10% and 57.73% with more marked increases at V5 in lutein, zeaxanthin, β-cryptoxanthin, β-carotene, and α-tocopherol. Obicetrapib 10 mg/day decreased non-HDL-C by 30.3%. In the non-HDL fraction at V5, obicetrapib 2.5mg significantly decreased lutein, zeaxanthin, γ-tocopherol, and α-tocopherol. At V5, obicetrapib 5mg significantly decreased γ-tocopherol and α-tocopherol. At V5, obicetrapib 10mg significantly decreased lutein, zeaxanthin, γ-tocopherol, and α-tocopherol. Obicetrapib 2.5mg, 5mg, and 10mg significantly decreased plasma oxLDL at V3 by 21.03%, 26.38%, and 22.00% and at V5 by 12.04%, 19.38%, and 18.85%.
Conclusions: Across doses, obicetrapib robustly increased lipophilic antioxidant levels. Despite a decrease in lipophilic antioxidants in non-HDL on par with LDL-C reduction, obicetrapib decreased oxLDL. These data reflect obicetrapib’s effect on non-HDL-C and support that, in fact, HDL protects against LDL oxidation.
4 Likes
Bicep
#168
I don’t understand the mechanism here. Where do the antioxidants come from? I understand the HDL is protective, so antioxidants are spared?
Well, since lutein and the like are not produced endogenously, presumably they must come from diet or supplementation. Not necessarily immediately, but from stores in tissues. Lipophilic antioxidants accumulate, so there’s something to draw upon.
It tells you in the abstract: they were shifted from the LDL and wider non-HDL cholesterol to the HDL-C (but still lowered oxLDL).
1 Like
adssx
#171
Great news! Assuming a standard review, obicetrapib could become available in the EU in late 2026/early 2027?
6 Likes
A_User
#172
Here’s the BROADWAY paper from earlier this year:
obicetrapib.pdf (439.2 KB)
5 Likes
Looks good. But also, we don’t have longitudinal data in clinical practice, 20-30 years like we have with statins. Pop a pill, cross your fingers (and pray, if that’s your pref). Given my abysmal and highly resistant lipids, I’ll be eating it like candy.
A_User
#174
Keep in mind the stock price jumped by around +34% after this study result, so if the PREVAIL trial that targets MACE reduction reports good results, pleiotropic, lowering MACE more than what is expected with the amount of LDL lowering. That could mean it might detect an all-cause mortality benefit, reduction in type 2 diabetes, etc. It could be a game changer then and data superiority of statins might not matter (although many will still probably take them at the same time). It’ll be quite some time until then and it will be approved for lowering LDL before that just like inclisiran.
7 Likes
A_User
#175
Even more data that lower is better, and obicetrapib is likely to work:
The cohort (mean age 66 years, 36% female, ASCVD 82%, HeFH 27%, diabetes 35%) had median baseline levels of low-density lipoprotein cholesterol (LDL-C) 92 mg/dL, HDL-C 48 mg/dL, apolipoprotein B (ApoB) 88 mg/dL, non-HDL-C 116 mg/dL, and lipoprotein(a) (Lp(a)) 40.5 nmol/L. Obicetrapib produced greater reductions in LDL-C (−34.0 vs −4.0 mg/dL, −37.8% vs −4.6%), ApoB (−19.0 vs −3.0 mg/dL, −21.7% vs −3.6%), non-HDL-C (−36.0 vs −4.0 mg/dL, −32.4% vs −3.7%), and Lp(a) (−9.8 vs 0 nmol/L, −32.5% vs 0%) and increased HDL-C (+68.0 vs +1.0 mg/dL, +140.0% vs +1.5%). The rate of coronary heart disease death, myocardial infarction, ischemic stroke, or coronary revascularization was lower with obicetrapib (3.9% vs 5.0%; HR: 0.77; 95% CI: 0.54-1.11; P = 0.16), with a risk reduction in the second 6 months (HR: 0.60; 95% CI: 0.37-0.99; P = 0.04). The rate of coronary heart disease death, myocardial infarction, or coronary revascularization was lower with obicetrapib (3.2% vs 4.7%; HR: 0.68; 95% CI: 0.46-1.00; P = 0.048), with a risk reduction in the second 6 months (HR: 0.45; 95% CI: 0.26-0.77; P = 0.003). Achieved levels of LDL-C (P = 0.003), ApoB (P = 0.007), non-HDL-C (P = 0.01), Lp(a) (P = 0.003), and HDL-C (P = 0.0001) were associated with event rates.
Impact of Obicetrapib on Major Adverse Cardiovascular Events in High-Risk Patients: A Pooled Analysis
6 Likes
Note that this analysis is confined to one year. It’s kind of astounding that they can cut events that quickly in a group whose starting apoB was already reasonable.
5 Likes
Clinical Development Updates
NewAmsterdam is developing obicetrapib, an oral, low-dose and once-daily investigational cholesteryl ester transfer protein (“CETP”) inhibitor, as the preferred LDL-C lowering therapy to be used in patients at risk of CVD for whom existing therapies are not sufficiently effective or well-tolerated.
- In July 2025, NewAmsterdam announced additional results from the prespecified Alzheimer’s disease (“AD”) biomarker analysis in the Phase 3 BROADWAY trial, presented at the 2025 Alzheimer’s Association International Conference (“AAIC”), which NewAmsterdam believes further support the potential of obicetrapib to modify key biomarkers of AD pathology over a 12-month period in patients with atherosclerotic cardiovascular disease (“ASCVD”).
- In ApoE4/E4 carriers, the highest risk category for Alzheimer’s disease, obicetrapib was observed to reduce p-tau217 levels by 20.5%, over 12 months, compared to placebo (p=0.010, n=29).
- In October 2025, the data was published in the Journal of Prevention of Alzheimer’s Disease.
- In August 2025, NewAmsterdam presented pooled efficacy and safety data from its pivotal Phase 3 BROADWAY and BROOKLYN trials at the European Society of Cardiology Congress (“ESC”) 2025, along with the simultaneous publication in the Journal of the American College of Cardiology, highlighting obicetrapib’s performance across diverse lipid-lowering backgrounds observed in these trials. The presentation and publication underscore the Company’s continued momentum in advancing obicetrapib as a differentiated oral therapy for patients with elevated LDL-C.
- In November 2025, NewAmsterdam expects to present additional data at the American Heart Association’s Scientific Sessions 2025, highlighting obicetrapib’s impact on LDL particles observed in BROADWAY and BROOKLYN.
Upcoming Milestones and Ongoing Trials:
Following the successful completion and positive topline results of the Phase 3 BROADWAY, TANDEM, and BROOKLYN trials, NewAmsterdam plans to announce additional data from these trials relating to obicetrapib and the FDC of obicetrapib plus ezetimibe.
The following Phase 3 trials are currently ongoing:
-
PREVAIL Phase 3 trial: PREVAIL is a CVOT evaluating obicetrapib in patients with a history of ASCVD, whose LDL-C is not adequately controlled despite being on maximally tolerated lipid-lowering therapy. NewAmsterdam completed enrollment of over 9,500 patients in April 2024.
-
REMBRANDT Phase 3 trial: The trial will utilize coronary computed tomography angiography imaging to evaluate the effect of obicetrapib plus ezetimibe FDC on coronary plaque. The placebo-controlled, double-blind, randomized, Phase 3 trial is being conducted in adult participants with high-risk ASCVD with evidence of coronary plaque who are not adequately controlled by their maximally tolerated lipid-modifying therapy, to assess the impact of the obicetrapib 10 mg plus ezetimibe 10 mg FDC daily on coronary plaque and inflammation characteristics. The trial is expected to enroll 300 patients.
NewAmsterdam also plans to initiate the RUBENS Phase 3 clinical trial to evaluate obicetrapib in combination with ezetimibe in patients with type 2 diabetes or metabolic syndrome that require additional lowering of LDL-C despite treatment with available therapy. The RUBENS trial is expected to initiate in the fourth quarter of 2025.
https://ir.newamsterdampharma.com/news-releases/news-release-details/newamsterdam-pharma-provides-corporate-update-and-reports-5?utm_source=li&utm_medium=organic&utm_campaign=earnings&utm_content=3q2025
1 Like