More on these updated European guidelines:
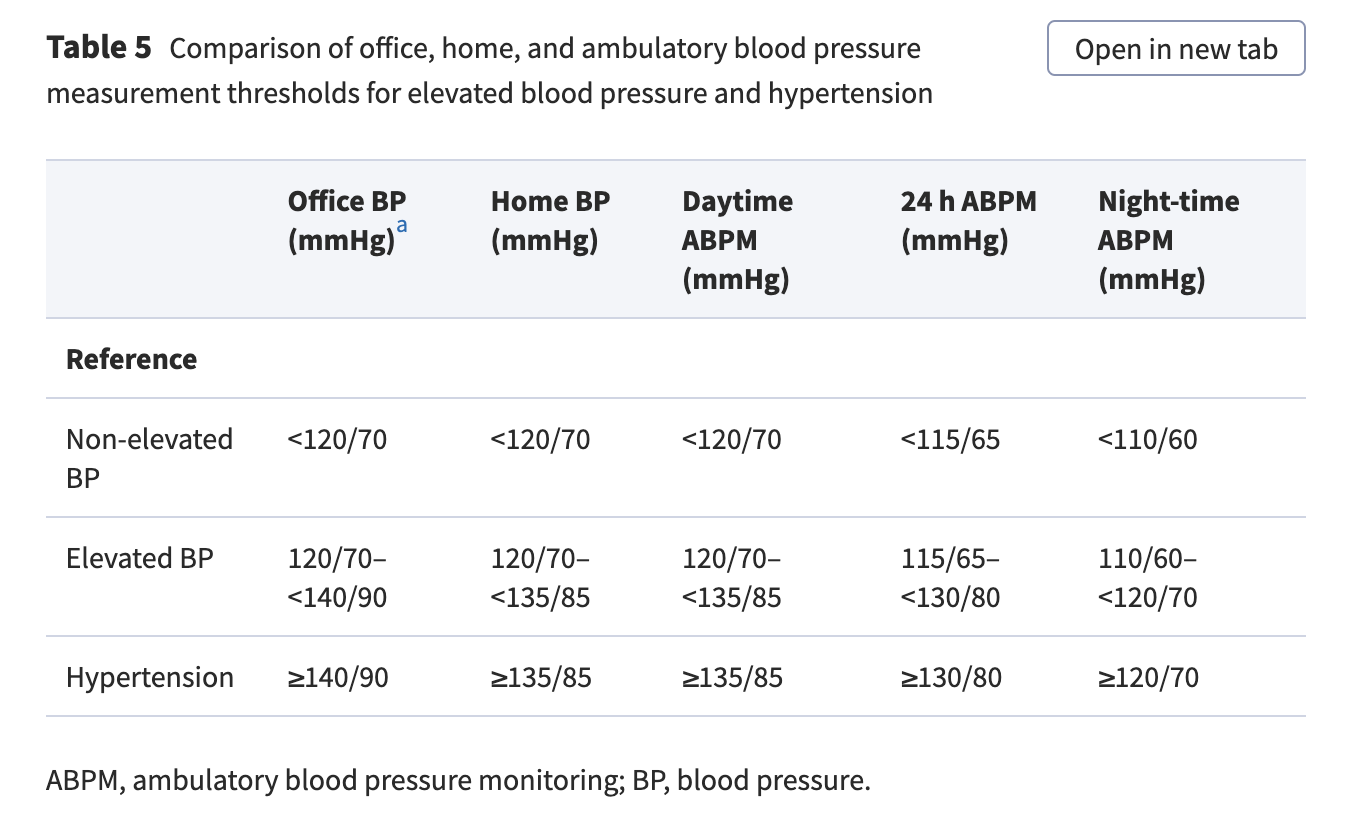
The “non-elevated” threshold for SBP is identical to the American guidelines but for DBP it’s even lower (70 vs 80 mmHg):
Protocol:

However, there is at present insufficient scientific consensus on the accuracy standards and validation procedures that these cuffless devices must comply with prior to commercialization. In view of these issues, none of these cuffless measurement modalities are currently recommended for routine clinical use.
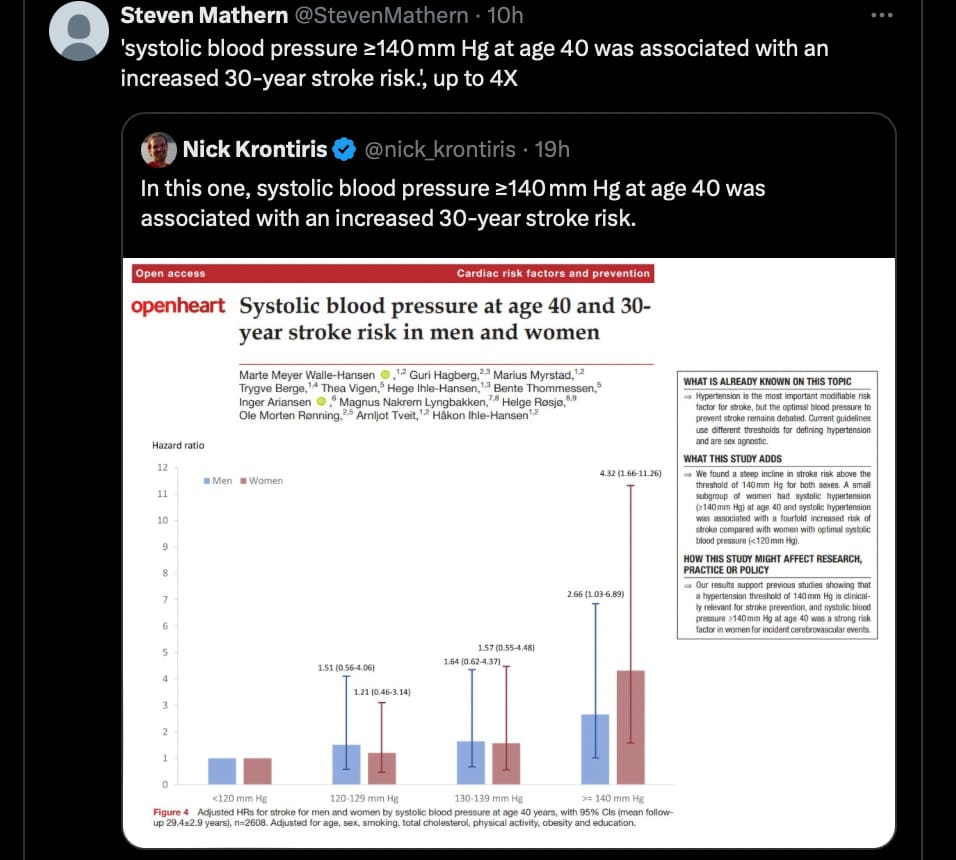
Epidemiological studies demonstrate a continuous and log-linear association between BP and adverse CVD outcomes. Starting at levels as low as 90 mmHg systolic, the higher the BP the higher the relative risk of CVD including atherosclerosis.
In compiling this categorization, priority was given to evidence from randomized trials over observational data. However, it is important to reiterate that the risk of CVD attributable to BP is continuous and that interpreting randomized trial data is an iterative process involving an element of subjectivity. As such, no categorization of BP can be considered immutable or flawless.

Here, we introduce a new BP category called ‘elevated BP’, which is defined as an office systolic BP of 120–139 mmHg or diastolic BP of 70–89 mmHg. Within this BP range, the efficacy of BP-lowering therapy has been established in meta-analyses of RCTs,but average CVD risk in the elevated BP group is not sufficiently high to merit drug treatment in all patients.
I was surprised they used “non-elevated”, they explain it:
Non-elevated BP is defined as a systolic BP of <120 mmHg and a diastolic BP of <70 mmHg. Fewer individuals within this BP range are at increased risk of CVD, and evidence for CVD benefit with BP-lowering pharmacological treatment is lacking due to an absence of trials. We use the term ‘non-elevated BP’ to define this BP category in recognition that these are treatment categories and not prognostic categories. Because the relative risk for CVD starts to increase at BP below this threshold (even as low as 90 mmHg systolic BP), particularly among women, we avoid terms like ‘normal BP’, ‘optimal BP’, or ‘normotension’ in defining this category.
Still:
Furthermore, research data indicate that, to optimally reduce CVD risk, achieving an on-treatment BP of 120/70 mmHg is the best point on the BP target range provided in our guideline recommendations
The lower the better…
In line with the latest research they recommend isometric resistance training:

On beta-blockers:
Beta-blockers and diuretics, especially when combined, are associated with an increased risk of new-onset diabetes in predisposed patients.
Beta-blockers should also be avoided in patients with isolated systolic hypertension or more generally with arterial stiffness, as they increase stroke volume (given the lower heart rate).
A vasodilating beta-blocker (e.g. labetalol, carvedilol, or nebivolol) is preferred when a beta-blocker is chosen.
The reason why beta-blockers are not considered first-line BP-lowering medications (outside of compelling indications) is not because of inferior BP-lowering properties (particularly for vasodilating beta-blockers), but because of inferior efficacy in reducing CVD events (particularly stroke) among patients with hypertension, and tolerance issues.
Low-dose combo is preferred:
Upfront low-dose combination therapy is therefore recommended in persons with hypertension, with the potential advantages of fewer side effects and swifter BP control being important for long-term adherence.
Isolated systolic hypertension in young adults (ISHY):
In young patients with isolated systolic hypertension, arterial stiffness and relative risk of CVD events appear to be similar to those without isolated systolic hypertension and lower than young adults with combined systolic-diastolic hypertension and isolated diastolic hypertension. Indeed, younger patients with isolated systolic hypertension appear to comprise a heterogeneous group. For these reasons, it might be reasonable to assess central BP and arterial stiffness in these individuals, as recommended by other scientific societies.
Orthostatic hypotension
However, the frequency of orthostatic hypotension is not increased in the more intensive BP-lowering arms of randomized trials compared with the less intensive BP-lowering arms. As such, and in contrast to common belief, it does not appear that more intensive treatment of BP (which almost always requires more BP-lowering medication) worsens orthostatic hypotension. In contrast, there is some evidence that more intensive treatment of hypertension may actually reduce the risk of orthostatic hypotension.
For dementia:
While one trial suggested superiority of long-acting CCBs, it is unclear if any first-line BP-lowering agent is preferable for preventing dementia and cognitive impairment.
Key messages:
The risk for CVD attributable to BP is on a continuous log-linear exposure variable scale, not a binary scale of normotension vs. hypertension.
Despite the growing number of hypertension guidelines, the rates of diagnosis, treatment, and control of hypertension (and elevated BP) remain suboptimal. A major factor underlying this is poor implementation of evidence-based guidelines in real-world clinical practice.
They also published a supplement with more details, they note:
Systolic BP appears to be a stronger determinant of CVD risk than diastolic BP.
Observational studies of community-based populations have reported that incremental pulse pressure is associated with an increased risk of CVD events, including coronary heart disease and heart failure. However, after adjusting for other BP parameters such as systolic BP, diastolic BP, or mean arterial pressure, pulse pressure is a weaker predictor of CVD events than these other BP parameters.
Related to this association between BP variability and risk, among patients on BP-lowering medication, time in target range seems to be the best measurement to predict the risk of major adverse CVD events. Nevertheless, the clinical role of BP variability in guiding treatment decisions appears limited, in particular because it has not been established that (i) the link between BP variability and CVD events is causal, and (ii) interventions specifically designed to reduce BP variability result in fewer CVD events, particularly over and above the effect of BP-lowering medication on mean BP value.