Looking at the original PDF it is a typo in the original PDF.
Dr. Greger is at it again, never missing an opportunity to promote WFPB.
The Role Meat May Play in Triggering Parkinson’s Disease (Dr. Greger)
A_User
#905
I liked this one more:
Are pawpaws safe to eat? Pawpaw fruits, like soursop, guanabana, sweetsop, sugar apple, cherimoya, and custard-apple, contain neurotoxins that may cause a neurodegenerative disease.
And the vegan version of Chris Masterjohn responds:
1 Like
adssx
#906
Mitochondrial damage triggers the concerted degradation of negative regulators of neuronal autophagy 2025
Here, we demonstrate that in response to mitochondrial damage in neurons, MTMR5, MTMR2 and Rubicon undergo concerted degradation in a graded manner, independent of Pink1/Parkin activity. Upon mitochondrial stress, we find that Rubicon is ubiquitinated and targeted to the proteasome for degradation; MTMR2 and MTMR5 are also ubiquitinated in response to mitochondrial stress, but their degradation involves both the proteasome and calcium-dependent proteolysis. We term the selective degradation of these proteins in response to mitochondrial damage as the Mitophagic Stress Response (MitoSR), and hypothesize that this response accelerates mitophagic flux by degrading the negative regulators of autophagy. Consistent with recent findings that MTMR5/MTMR2 negatively regulate autophagosome biogenesis48, we find that loss of this myotubularin complex enhances mitochondrial engulfment in response to oxidative damage in neurons. In contrast, under basal conditions, Rubicon is recruited to neuronal lysosomes via RAB7, blocking lysosomal function and thereby inhibiting autophagosome maturation. We find that targeted depletion of these negative regulators significantly increases mitochondrial turnover in neurons under both basal conditions and upon induction of mild oxidative stress. Thus, we propose that therapeutic interventions directly targeting negative regulators of autophagy may promote clearance of damaged mitochondria in patients suffering from neurodegenerative diseases such as PD and ALS, where mitophagy is compromised.
1 Like
In the end if the mitochondria are not functioning well enough the cell cannot produce the proteins for autophagy.
3 Likes
adssx
#908
There’s an ongoing trial of MK7 in PD but I’m afraid we might never get the results. Meanwhile, mechanistic studies look good: Menaquinone-7 - an interesting molecule to power up the mitochondria - #80 by adssx
1 Like
adssx
#909
Mendelian randomization preprint from McGill University: Investigating the genetic relationship between vitamin B12 deficiency and Parkinson’s disease 2025
Our analysis showed no associations between common variants of genes crucial in B12 metabolism and PD. Pathway PRS identified nominal association between B12-related genes and PD (OR = 1.061, 95% CI: 1.004–1.121, p = 0.038), which did not survive Bonferroni correction. In the rare variants analysis, we identified a significant association between variants with high CADD scores in the CUBN gene (P=6.07E-05; Pfdr=0.005) in the AMP-PD cohort, driven by the benign variant p.G3114S (OR=3.3; p=3.56E-05); however, this was not validated in the meta-analysis. We did not identify a potentially causal relationship between vitamin B12 levels and the risk, age-at-onset, or progression of PD. Additionally, no genetic correlation was observed between vitamin B12 and PD risk or age-at-onset GWASs.
Confirmed by two previous MR studies:
Bidirectional two-sample Mendelian randomization analysis identifies causal associations between oxidative stress and Parkinson’s disease 2024
As for PD, the IVW method suggested that the Zinc (Zn) levels was significantly associated with PD (OR = 1.107, 95% CI 1.013–1.211; p = 0.025), which is consistent with results from the weighted median analyses. Moreover, the results remained consistent and robust in the sensitivity analysis. However, there were no significant associations of catalase, glutathione peroxidases, superoxide dismutase, vitamin A, vitamin C, vitamin E, vitamin B12, folate, copper, or iron with PD. As for OS, our reverse MR analysis also did not support a causal effect of liability to PD on OS.
Investigating the causality of metabolites involved in one-carbon metabolism with the risk and age at onset of Parkinson’s disease: A two-sample mendelian randomization study 2021
In addition, we did not observe any evidence that the circulating levels of vitamin B6, vitamin B12 and folate acid affected the risk of PD or age at onset of PD. Our findings implied that lowering homocysteine levels through vitamin B6, vitamin B12 or folate acid supplementation may not be clinically helpful in preventing PD or delaying the age at PD onset.
On the other hand, this abstract found: Higher Serum Vitamin B6 and B12 Levels Associated with Parkinson’s Disease Incidence (P2-5.003) 2025
“2,757 participants (mean age 59.7[SD, 12.4], 45.8% men) followed on average for 19.4[SD, 6.1] years were included. With surveillance beginning 5 years after entry, there were 40 incident PD cases. The highest tertiles of serum B12 (HR 2.27 [95% CI 1.04, 4.95], p=0.040) and B6 (HR 2.96 [1.24, 7.07], p=0.015) levels were associated with incident PD, but not vitamin intake. Higher serum vitamin levels were not associated with incident dementia or Alzheimer’s disease. Higher dietary intake of vitamins was not associated with incident PD.”
So B12 supplementation is irrelevant in PD? (poke @DrFraser)
4 Likes
The way this is presented, one would think that pre-existing B12 levels being high were a risk for PD, but if you happen to be taking some supplements, that didn’t worsen things - which mechanistically is interesting and a bit counter-intuitive. However, supplementation isn’t always the same thing as lifestyle or other genetics resulting in a higher level.
I very much appreciate the laser focus on PD … and overall, I think exercise, including things with a lot of balance and aerobic activity (pickleball for us elders), some weight training, 40 hz devices and GLP-1s are among the the things to highly consider (I know there are more).
But in conjunction with this, if one has a Homocysteine of 35 … I’d still treat it - but for other reasons, just not in the delusion that this will impact PD.
Neurodegeneration will remain a tough nut to crack.
3 Likes
I wonder if SS 31 / Elamipretide would help with this?
I keep getting delayed in my experiment with this peptide, been quite busy the past couple of weeks
https://www.sciencedirect.com/science/article/pii/S0753332225002501
Contemporary insights into elamipretide’s mitochondrial mechanism of action and therapeutic effects
Highlights
• Mitochondria electron transport system (ETS) produces essential cellular energy.
• ETS is located on cardiolipin (CL)-rich cristae of inner mitochondrial (MITO) membrane.
• In disease, elamipretide binds to CL, improving MITO structure, function and dynamics.
• In animals, elamipretide improves MITO function in cardiac and skeletal myopathies.
• In humans, elamipretide improves symptoms of Barth syndrome myopathy
1 Like
adssx
#912
There’s zero evidence that homocysteine-lowering interventions help with anything other than stroke. ZERO: What are your homocysteine levels? What have you done to reduce it? Why isn't it part of PhenoAge or aging.ai clocks? - #156 by adssx
So homocysteine is probably a sign (consequence) of something else going wrong (hard to know what!), but treating it won’t bring benefits.
3 Likes
Homocysteine’s interference with the NO chain via ROS is more than enough reason to crush it.
It isn’t just a signal of bad stuff; it is bad stuff.
adssx
#914
So how do you explain that Mendelian randomization studies don’t find any causal effect for any diseases other than stroke? And how do you explain that homocysteine-lowering RCTs failed for most conditions? Is there strong evidence (RCT + MR) in favor of homocysteine lowering interventions for anything other than stroke? I’m not talking about longitudinal association studies.
1 Like
A_User
#915
Serum B12 isn’t specific enough for B12 deficiency and the effects might be non-linear and MR is not good for detecting non-linear effects (i.e a threshold where risk increases, like where the percentile that causes deficiency has negative effects, maybe 1-10th percentile lowest B12 – the rest above no effect).
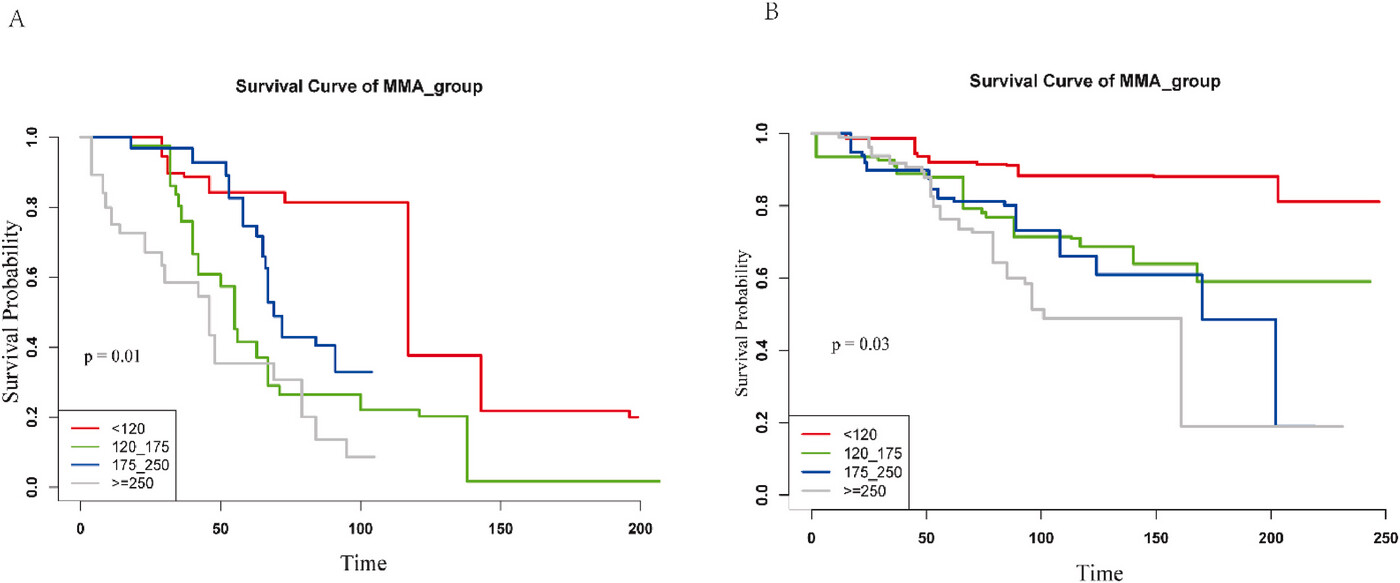
I searched for methylmalonic acid (but the authors didn’t mention B12):
A non-linear correlation was observed between MMA and AD-specific death and PD-specific mortality. The presence of MMA Q4 was linked to increased death rates among AD patients (HR = 6.39, 95%CI: 1.19–35.24, P = 0.03) after controlling for potential confounders in a multivariable weighted Cox regression model. In PD patients, the MMA Q4 (Q4: HR: 5.51, 95 % CI: 1.26–24, P = 0.02) was also related to increased mortality. The results of survival analysis indicated that the poorer prognoses were observed in AD and PD patients with MMA Q4
https://www.cell.com/heliyon/fulltext/S2405-8440(24)05388-X
adssx
#916
Yes B12 deficiency is bad. Any deficiency is. It is also possible that the current threshold for deficiency is a bit too low. But once/if you’re above that threshold, the evidence for B12 supplementation seems to me very weak. It’s at best association studies. And even some association studies found detrimental effects: Parkinson's disease - #909 by adssx
I would love to be proven wrong.
2 Likes
adssx
#917
Also, B12 supplementation might be beneficial in people with PD already on levodopa due to some effects of levodopa, see:
And:
https://www.prd-journal.com/article/S1353-8020(23)00080-9/abstract
2 Likes
I don’t really care to tell you the truth. I just want add much NO and endothelial protection as possible. I don’t see how you could argue against it. Absence of evidence is not evidence of absence I guess, at least for me.
adssx
#919
Then you should consider joining another online community because the goal here is to learn together and find the truth. If you just want to affirm things without spending time reviewing the evidence, go to TikTok.
3 Likes
No doubt we should look for truth, but sometimes you just have to take the available evidence and make a leap of faith. We all may be dead until something is known for certain. This is a Rapamycin forum, isn’t it? Despite the lack of long term human trials, we have taken that logical leap.
adssx
#921
Of course, we all make decisions under uncertainty. The evidence in favor of B12 supplementation in people without B12 deficiency to prevent PD is just not there.
@adssx 's point is that people should evidence their argument rather than “make a leap of faith”.
B6, 9 and 12 are interesting in lots of ways. However, B6 particularly has a u shaped curve because of self-inhibition, B9 personally I think the normal range may be actually below optimal values.
B12 I don’t think have evidence for oversupplementation.
1 Like