L_H
#2503
Ok, but I’ve never seen a study (statin or pcsk9i) which gives decent data on the advantage of targeting Apob so low. Care to share? I’m keen to follow the science on this.
@SNK This is interesting. I think you are finding important info for yourself that could be useful to me as well. I also seek that sweetspot …. For me I look for high benefit (slowing aging and maintaining recovered function) without much cost beyond feeling tired for a day every week or so. I’m not looking to gather additional benefit on ann unverified assumption that feeling poorly will payoff in the long run. It might, I admit but I’ll wait for more information.
2 Likes
L_H
#2505
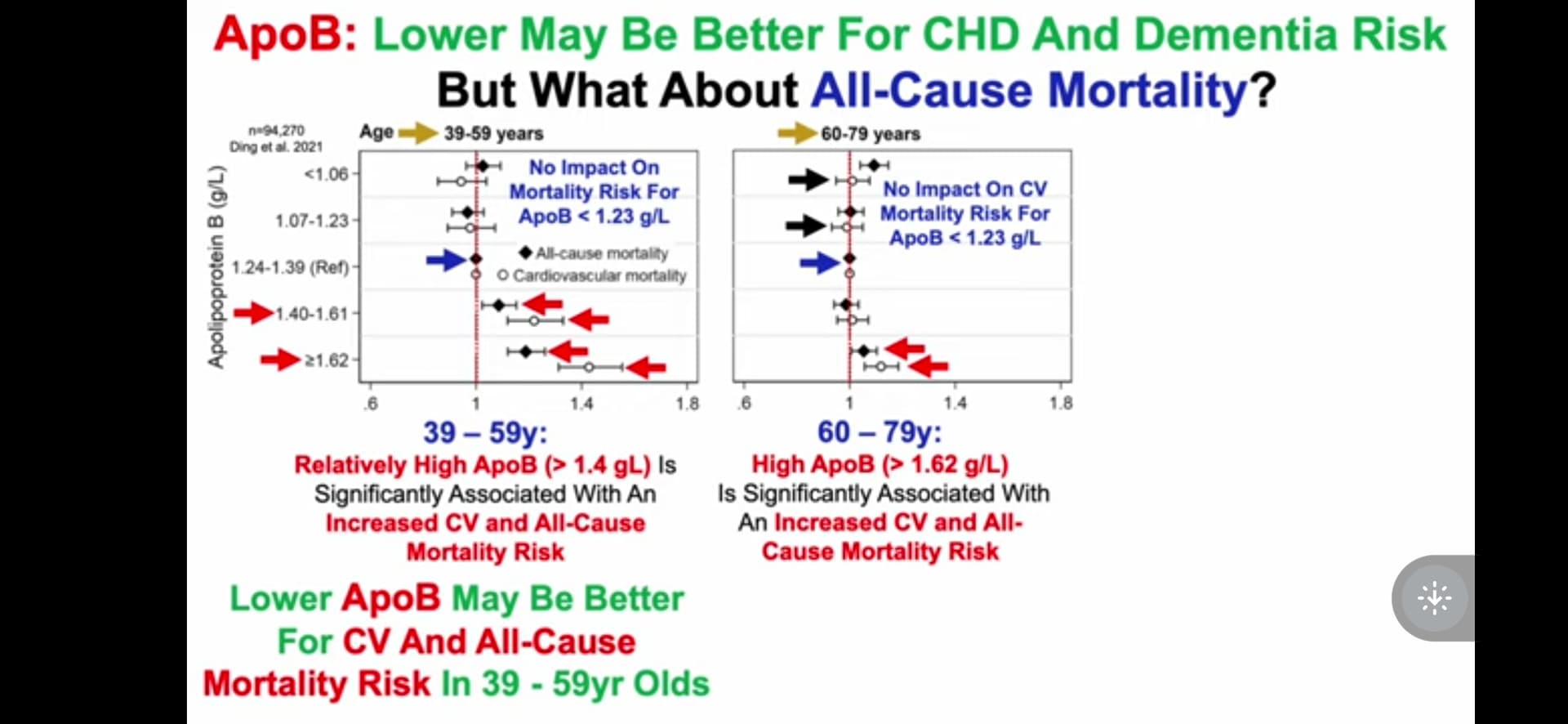
Hi, there seems to be some evidence that apob vs all cause mortality is u-shaped.And ditto for dementia risk. But I’m not totally convinced we know where the sweet spot is, or even if that’s correct.
https://www.sciencedirect.com/science/article/abs/pii/S0002962923013162#:~:text=ApoB%20was%20linearly%20associated%20with,of%20other%20cardiovascular%20risk%20factors.
3 Likes
Just thinking creatively for a moment, it does seem that everything we do naturally (eat, hydrate, breath, move, sleep …not including injections into blood stream or injuries or bullets) come with a sweetspot. Extremes tend to be the exception. But…when dealing with a damaged organism (an older person who has accumulated problems), it’s hard to understand how that might change. If I have some damage to my endothelium, maybe I need to act more aggressively to slow the rate of damage, as an example. This is what I am wondering. In the meantime I am acting aggressively to stay/get to a lower position on apoB / HbA1c.
2 Likes
jnorm
#2507
I just started rapamycin a couple weeks ago at 29, and I plan to test ApoB and lipid levels here soon. Before starting, my triglycerides last tested at 58 and LDL at 95. I definitely would like LDL to be a bit lower, so I’m going to play around with diet.
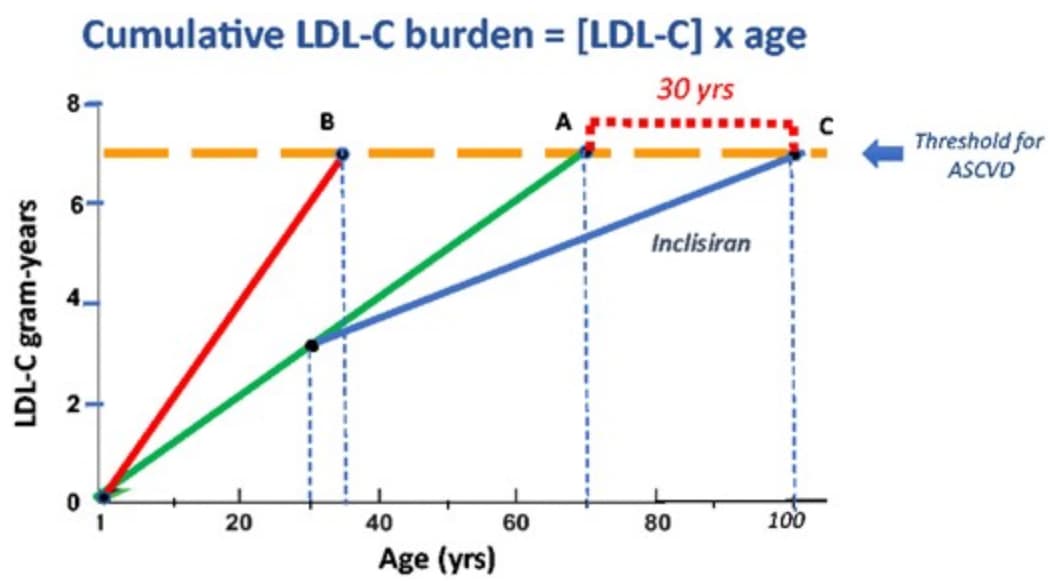
Recently I came across the short paper How to live to 100 before developing clinical coronary artery disease: a suggestion, where atherosclerotic burden is related to ‘LDL-C years’.
Line A represents a person with an average level of LDL-C of 100 mg/dL (2.6 mmol/L) either naturally or on a statin, who reaches the ASCVD threshold of 7 LDL-C gram-years at the age of 70 years. Line B represents an untreated patient with familial heterozygous hypercholesterolaemia with an LDL-C of 200 mg/dL (5.2 mmol/L), who reaches this threshold at the age of 35. My suggestion is to administer 300 mg of inclisiran once each year, beginning at the age of 30 years, to subjects represented in Line A. As a consequence, their LDL-C would fall from 100 to 60 mg/dL (Line C), the rate of progression of the atherosclerotic burden would decline, and the threshold of 7 gram-years would be reached 30 years later, when the subject reached the age of 100.
3 Likes
A_User
#2508
That is because of reverse causation.
Here’s the studies you asked for, LDL is highly correlated with apoB.
Statins:
PCSK9 inhibitor:
https://www.nejm.org/doi/full/10.1056/nejmoa1615664
Bonus:
We provide mechanistic insight for this effect by showing that approximately 42% of the causal effect of LDL-c on lifespan is mediated through pathways independent of CAD and ischaemic stroke. This is consistent with the observation that LDL-c has a causal effect on a range of outcomes beyond CAD, including peripheral vascular disease46, 47 and abdominal aortic aneurysm.
https://bpspubs.onlinelibrary.wiley.com/doi/10.1111/bcp.14811
Bonus two:
https://www.thelancet.com/journals/lanhl/article/PIIS2666-7568(21)00086-6/fulltext
1 Like
Neo
#2509
As discussed on this forum before (you can search), there is also
(A) gold standard Mendelian randomization evidence
(B) the fact pattern that young humans even during development of the brain have lower apoB than middle age adults (and that evolution did not have incentives to optimize longevity or health post the most common historical reproductive age)
1 Like
A_User
#2510
What an aboslute 94 year old clear-thinking, forward-thinking, legend!
SNK
#2511
A bit off topic here (but since you brought it up) I have always been puzzled why human reproductive age has such a huge gap between males and females, whereas in all (or at least most) animals I know of there is little or no difference at all? Would be interesting to see if any scientists ever tried to explain this. Reason i bring it up is because somewhere somehow (in my brain) I think that what works for men, may not work for women (for the most part) when it comes to longevity.
Virilius
#2512
The U-shape observational studies have been superseded by trials like JUPITER which showed a big reduction (-20% from 1.25 to 1.0) in all cause mortality in the rosuvastatin group compared to placebo. Do not trust observational studies until Mendellian randomization proves causation!
1 Like
Virilius
#2513
Fertility rates drop off for males too after the age of 40. Maintaining good sperm quality requires exercise and supplementation.
L_H
#2514
I thought the JUPITER trial was looking at the impact of rosuvastatin on men with median 108 mg/dL ldl-c. So quite a bit higher. Was there sub- analysis showing benefit below 50/60 mg/dl?
L_H
#2515
Hi, what are you targeting for apoB and hba1c?
1 Like
L_H
#2516
I like this, and i hadn’t read it.
I’ll go through it now
SNK
#2517
What you said has nothing to do with what I was saying. There was a 93 year old man that had a baby with his 32 year old wife a while back, and I think good old Al Pacino at 83 had a baby also.
1 Like
Virilius
#2518
If LDL-C can be kept very low from birth, atherosclerosis will not occur.
“initiating lipid-lowering therapy after a person has already been exposed to a cumulative burden of 6250 mg-years of LDL by age 50 years means that person has very likely already developed a large atherosclerotic plaque burden … lowering LDL after this cumulative exposure to LDL should reduce the risk of cardiovascular events, but this person will remain at relatively high “residual” risk of experiencing an acute cardiovascular event because one of the underlying plaques can still disrupt to cause an acute coronary syndrome
Humans were never meant to harbor the low-density lipoprotein cholesterol (LDL-C) levels that are now commonplace. In one series of 147 full-term neonates, the average LDL-C was 20 ± 10 mg/dL [59] Despite the extraordinary rate of development and need for myelination, even neonates need very little LDL-C
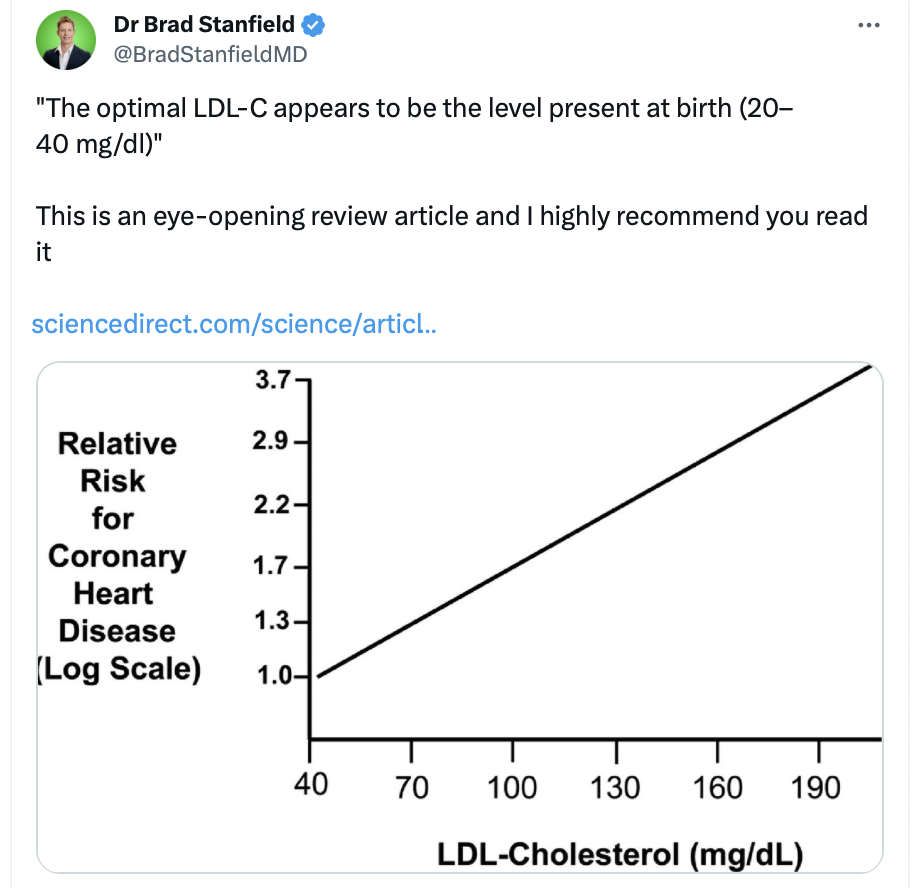
a ‘normal’ non-atherogenic LDL-C level is 20–40 mg/dl.
Based on the log-linear relationship of LDL-C to the hazard ratio for an acute ASCVD event, the LDL-C level where no excess risk occurs is approximately 38 mg/dL or 1 mmol/L
Dr Brad Stanfield auf X: „“The optimal LDL-C appears to be the level present at birth (20–40 mg/dl)” This is an eye-opening review article and I highly recommend you read it https://t.co/eUn5FZUPs5 https://t.co/KvBCXVnupc“ / X (twitter.com)
2 Likes
L_H
#2519
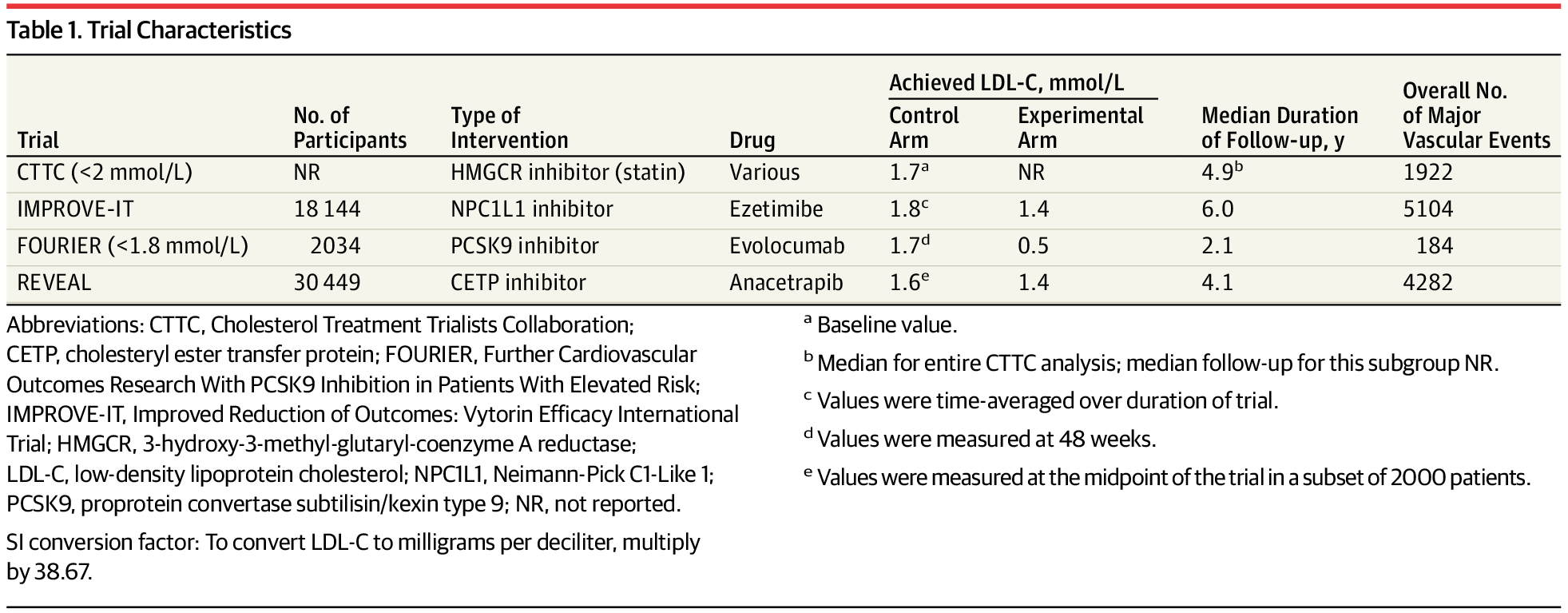
I’ve just spotted some issues. This doesn’t look at the impact of statins, and is for secondary prevention only.
“nonstatin LDL-C–lowering therapy added to background statin therapy were included in the meta-analysis (Table 1). All 3 were secondary prevention trials that enrolled patients with known atherosclerotic cardiovascular disease.”
I like Peter Attia’s analogy that if you leave it until you’ve acvd, then you need to slam on the brakes. That’s what seems to be happening here.
Of the three rcts it references I’m familiar with two look at the third now
A_User
#2520
It is citing this study:
Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170 000 participants in 26 randomised trials
https://www.thelancet.com/action/showPdf?pii=S0140-6736(10)61350-5
1 Like
A_User
#2521
Is it possible to buy this drug from chemical synthesis?
https://www.nejm.org/doi/full/10.1056/nejmoa1706444
Anacetrapib, CETP inhibitor (-18% apoB, +36% apoA1)
2 Likes
A_User
#2522
1 Like