I do remember a study where 5mg every day had a slightly higher LDL reduction than 20mg every other day.
1 Like
scta123
#2544
Have you looked at cyclodextrin?
LaraPo
#2545
Just looked it up - there’s Alpha and Beta - cyclodextrin. Which one?
Davin8r
#2546
I switched to putting a tablespoon of organic amla powder in my daily smoothies for a long time, but recent blood work showed no apparent effect, so last month I switched back to the TrueCapros and will be getting repeat lipid tests in a few weeks. Will let you know!
2 Likes
A_User
#2547
I saw a study awhile ago that 5 mg every day had about a 7% improvement in LDL over 10 mg every other day.
1 Like
scta123
#2548
Beta. But do a forum search there is more info in some posts.
1 Like
Neo
#2550
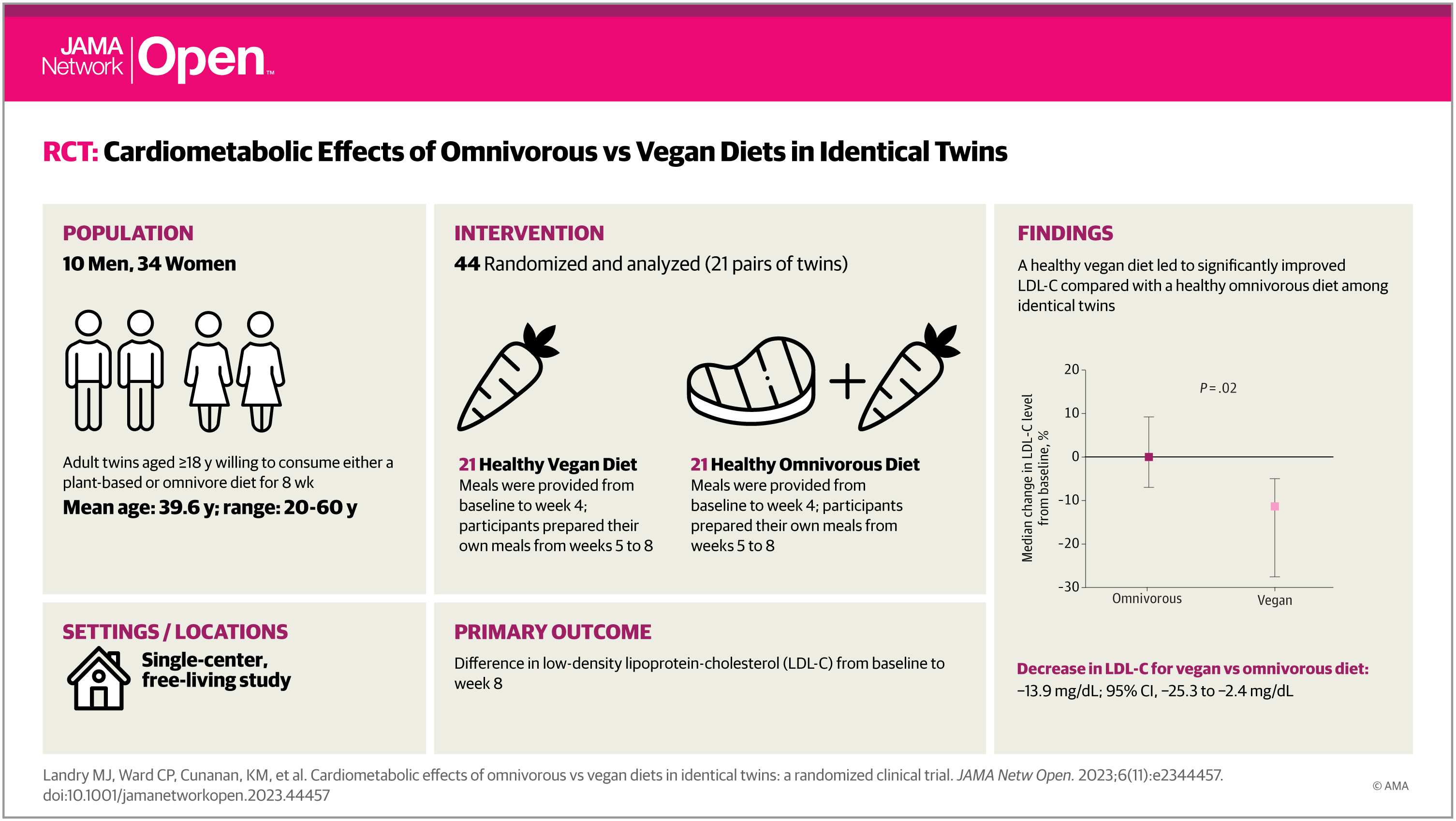
Interesting, strong trial design, out of Stanford and just published in JAMA
November 30, 2023
Cardiometabolic Effects of Omnivorous vs Vegan Diets in Identical TwinsA Randomized Clinical Trial
They also say
“twins on the vegan diet tested younger on measures of biological versus chronological age, data which will be presented in a future study, Gardner said.” per CNN
2 Likes
A_User
#2551
I did see that study but I heard it was an ad libitum study where they ate as much as they wanted, thus the vegan diet were in a caloric deficit which might explain some of the effect.
3 Likes
scta123
#2552
Diet-specific meals were provided via a meal delivery service from baseline through week 4, and from weeks 5 to 8 participants prepared their own diet-appropriate meals and snacks.
But still if ad libitum healthy vegan diet provides only caloric deficit it is surely worth considering it as a preventative measure.
2 Likes
L_H
#2553
Yes, this is a small study, but it’s encouraging that rosuvastatin eod had a bigger impact on triglycerides than rosuvastatin ed. Impact on ldl-c was comparable. And that’s with the same dose. Ie the every other day group had half the total mg.
I think my plan will be to test 2.5mg of both rosuvastatin and ezetimibe eod.That fits with pill sizes…
https://www.ijbcp.com/index.php/ijbcp/article/view/635
1 Like
Neo
#2554
Why ezetimibe eod? (Extra characters)
How Low Should You Go? Is Very Low LDL-C Safe?
Dec. 1/23 article …
Cognitive Function
The hypothesis that low LDL-C causes cognitive decline has been investigated prospectively in the EBBINGHAUS study, which included a subgroup of patients in FOURIER (evolocumab). Cognition did not differ in patients randomized to receive evolocumab compared with placebo as assessed by the Cambridge Neuropsychological Test Automated Battery. Among patients assigned to receive evolocumab, cognitive function did not differ in those with low LDL-C (< 25 mg/dL [< 0.6465 mmol/L]) and higher levels of LDL-C. The caveat of this study is that median treatment was 19 months. Reassuringly, in FOURIER-OLE — a longer-term, open-label follow-up study that switched placebo-treated patients in the parent trial to evolocumab — there was no trend toward an increase in neurocognitive events during a maximum exposure to evolocumab of 8.4 years and mean LDL-C of 30 mg/dL (0.7758 mmol/L). There was no concurrent use of placebo during this follow-up trial.
Clinical Trials: Benefits of Achieving Very Low LDL-C
Overall, contemporary clinical trials of combination lipid-lowering therapy have generally shown greater CV risk reduction down to LDL-C levels < 25 mg/dL (< 0.6465 mmol/L), without any lower safety limit for LDL-C levels. Some of the strongest evidence comes from the FOURIER trial, a randomized, double-blind, placebo-controlled trial evaluating subcutaneous evolocumab (140 mg every 2 weeks or 420 mg monthly) vs placebo in 27,564 patients with atherosclerotic CV disease and a baseline LDL-C of 70 mg/dL (1.8102 mmol/L) on statin therapy. There was a 59% average reduction in LDL-C levels at 48 weeks with evolocumab compared with placebo — LDL-C reduction from baseline of 92 mg/dL to 30 mg/dL (2.379 to 0.7758 mmol/L).
Over a median follow-up of 2.2 years, evolocumab reduced the risk for major adverse cardiovascular events compared to placebo (9.8% vs 11.3%; HR, 0.85; 95% CI, 0.79 to 0.92; P < .001). These results were consistent for secondary endpoints and across key subgroups, without a significant difference between groups with respect to adverse events other than injection-site reactions (2.1% in the evolocumab group vs 1.6% in the placebo group). Of note, although the average LDL-C on treatment was 30 mg/dL (0.7758 mmol/L) in FOURIER, many patients had on-treatment LDL-C levels < 10 mg/dL (< 0.2586 mmol/L). These are valid LDL-C values because FOURIER performed ultracentrifugation on low LDL-C, giving confidence that these individuals truly had such low LDL-C levels (with subsequent validation of the Martin-Hopkins equation in this group). Moreover, there was no increase in adverse events — only additional CV benefit — in participants who achieved such low LDL-C. The ODYSSEY Outcomes trial results are generally consistent with FOURIER but were not as robust in demonstrating the safety of low LDL-C owing to dose adjustments in therapy that led to less achievement of very low LDL-C and more variable LDL-C levels.
The Way Forward
The several lines of evidence presented support the safety of very low levels of LDL-C (ie, < 25 mg/dL [< 0.6465 mmol/L]). Therefore, there is no compelling reason to reduce doses of lipid-lowering medications in adults with LDL-C < 25 mg/dL [< 0.6465 mmol/L]). Clinicians should reassure patients that such low levels are not only safe but beneficial. Lowering LDL-C for longer better protects patients from CV events such as myocardial infarction and stroke
Artigo completo aqui:
https://www.medscape.com/viewarticle/998670
7 Likes
A_User
#2557
Yes, I actually didn’t care about drugs and statins at all before I saw similar evidence since I thought lifestyle could get everyone down to ~70 mg/dl.
I can’t speak for anyone else but that was convincing to me.
1 Like
Neo
#2558
Very compelling synthesis. Thanks @RapAdmin
After having had a break for a while, a month ago I re-started taking repatha and this time 2 x a month instead of just once a months. This paper strengthens my view that I made the right decision there.
(Also got a prescription for Eze that I might combine in if ApoB does not fall enough on the 2x Repatha a month (I’m more a re-absorber than producer, but may later consider adding a statin instead of Eze as an alternative to combine with the Repatha))
(My other issue is that have genetically non-optimal Lp(a) levels and have had non-optimal Homocysteine levels (thought think I’ve gotten that down to more optimal levels now via B6, 9 and 12 combo).
1 Like
Neo
#2559
Base editing, a new form of gene therapy, sharply lowers bad cholesterol in clinical trial
Verve Therapeutics says its twist on CRISPR could with one treatment help prevent heart disease, a major killer, in many people
https://www.science.org/content/article/base-editing-a-new-form-of-gene-therapy-sharply-lowers-bad-cholesterol
Neo
#2560
Endurance exercise and atherosclerosis
Is working out too hard detrimental to heart health?
https://twitter.com/b_holmer/status/1731289691503177741?s=46&t=zJMJ1xVdRJYEDYz-DHipTw
2 Likes
L_H
#2561
Just to so i don’t have to cut the pill into 8ths really. The half life is 22 hours, so the pharmokinetics will be a but bumpy. But given my low dose im guessing that wont have a large impact on AUC and therefore impact on apoB compared to daily dosing.
1 Like
L_H
#2562
Apologies if this has been raised before but there is some question mark over misclassifications in the fourier trial.
1 Like
L_H
#2564
Thanks Anuser, i read through the posts and something that seems to be missing is, regardless of how cardiovascular deaths were categorized, the evolocumab group had a slightly higher all cause mortality than the placebo group.
Given also that the subjects had cvd, this doesn’t at all seem like compelling evidence to target very low ldl-c in a healthy population.
1 Like