@rivasp12
Reviewing this paper you posted:
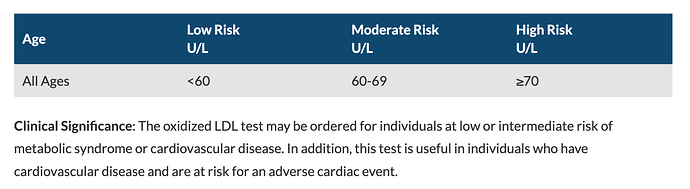
mTOR Inhibition and Cardiovascular Diseases Dyslipidemia and Atherosclerosis (2018)
The authors state “Furthermore, the risk of CVD is not higher in renal or liver transplantation patients receiving rapalogs despite significant dyslipidemia triggered by the treatment”
And the two references in support of this statement:
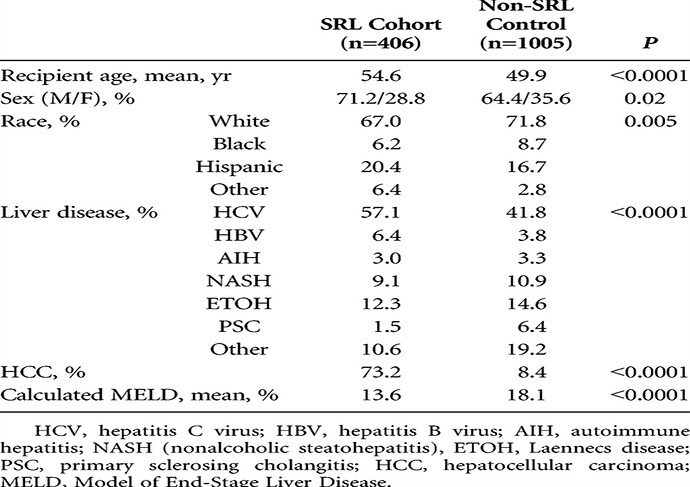
Sirolimus and Cardiovascular Disease Risk in Liver Transplantation
"We reviewed all 1812 liver recipients who underwent transplantation from 1998 to 2010, identifying a cohort using sirolimus as part of the initial immunosuppression (SRL Cohort) and a control group of the remaining patients from this period where SRL was never given (Non-SRL Control).
Conclusions. Sirolimus causes hypertriglyceridemia and hypercholesterolemia, but it does not increase the incidence of MI or other CVDs. Considering the SRL Cohort has more cardiac risk factors and nearly double 10-year predicted CVD risk, the fact that the CVD incidence is similar suggests that sirolimus is in fact cardioprotective."
2nd reference:
Cardiovascular risk in kidney transplant recipients receiving mammalian target of rapamycin inhibitors
https://sci-hub.se/10.1016/j.transproceed.2011.08.009
" The incidence of coronary artery disease was higher among patients treated with mTOR inhibitors (P .04). CVD, defined as myocardial infarction, percutaneous coronary intervention, stroke, aortic aneurysm, pulmonary thromboembolism, sudden cardiac death appeared in 26 study group compared with four control patients (P .24). The risk of any CVD was not significantly higher
among patients receiving mTOR inhibitors hazard ratio 1.94; 95% confidence interval 0.83– 4.52). In conclusion, no correlation was observed between the duration of mTOR
therapy and CVD"
Yet, some “concerning comments” in the discussion. Not a statistically mediated dismissive study?
“We observed more cardiovascular events among patients treated with mTOR inhibitors, although the incidence was not significantly more common compared with a control group; it was not affected by the duration of therapy. The risk of occurrence of a cardiovascular event was nearly twice as great in those recipients treated with an mTOR inhibitor, but it did not reach significance. We did noticed a higher incidence of coronary artery disease during mTOR inhibitor therapy. mTOR inhibitors have proven effects on hypercholesterolemia and hypertriglyceridemia in renal transplantation. Our study confirmed their detrimental influence”