FWIW: Rapamycin raised my albumin levels from 39 g/L to 44 g/L in a little over one month when I was taking my highest dosages of rapamycin. 10 to 20 mg biweekly with grapefruit juice.
That takes me from the hazard zone to the neutral zone. I am anxious to see my blood work in a couple of weeks after 8 weeks since my last dose of rapamycin.
https://www.ahajournals.org/action/downloadSupplement?doi=10.1161%2FATVBAHA.119.313681&file=atvb_atvb-2019-313681d_supp1.pdf
1 Like
I believe this is a one-off for whatever reason. I can find no supporting articles after a quick search to indicate that rapamycin increases serum albumin. In fact quite the opposite.
1 Like
Bicep
#571
I have 6 years of albumin numbers before Rapa and 3 since. 43.6 average before and 41.3 since. So it went down a little. It doesn’t bounce around much really. Going by the graph I may be a little high, but not much.
2 Likes
I take finasteride, so I can’t donate blood.
Yet another reason I need to get on the ball and strike it rich so I can have my own blood boy.
1 Like
Bicep
#573
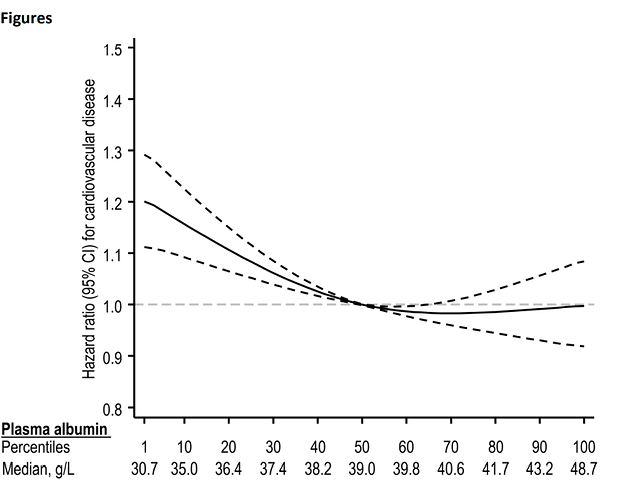
I’m still looking at the graph above. It looks like you want your albumin to be between 39 and 48 with optimal around 40. Can anybody explain why the line goes up above 40? In the book Malcolm says normal is between 35 and 55. What happens above 48.7? Why does the graph stop?
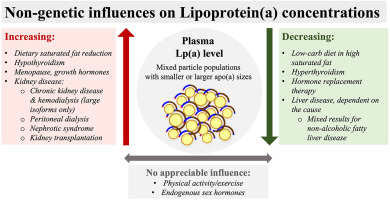
The lipid du jour is Lp(a). This has been shown to be a fairly significant coronary risk factor, kind of up there with ApoB.
It looks like statins don’t really affect it, but you can rather significantly lower it with saturated fats and androgenic steroids. No effect with exercise.
Interestingly, when Lp a goes down, LDL goes up.
So I guess after I get my LDL down with lots of statins, I’ll gorge myself with saturated fats and shoot up with androgenic steroids.
Then I’ll be just right!
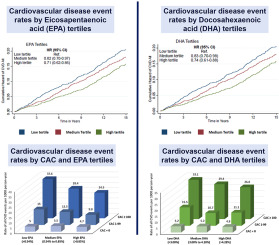
And after engaging in that useless endeavor I’ll actually do something worthwhile and check a coronary calcium score. If elevated, omega3’s can significantly alter the CVD event prognosis.
MAC
#575
What Kendrick book do you refer to?
Ok, thats a VERY weak causation science by Malcolm.
And the mortality graph (hazard ratio vs plasma albumin) posted above shows a relatively weak all cause mortality graph, which of course includes CVD?
Can you be our mouse and do this experiment? And add inflammation markers before and after if you don’t already: 
Seems albumin is pretty tightly controlled in healthy individuals…and this low albumin association could be one of those confounders, like low LDL-C and mortality. And maybe it’s all about the QUALITY (glycation, impact on glycocalyx, other inflammatory pathways, plasma transfusions research) of the albumin that is causative, and not qty per se.
1 Like
Michael Lustgarten, Ph.D., has an interesting video about albumin levels on Youtube.
Yours looks pretty good.
Albumin: What’s Optimal For Youth And Health? (2022 Update)
3 Likes
Albumin seems to be basically a marker of inflammation. With inflammation the body makes more of certain proteins like c reactive protein, but there’s then a correspondent decrease in its production of albumin.
MAC
#578
I like this mechanism, this make more intuitive sense to me. I think I’m going to throw in IL-6 and TNalpha on my next panel, so I have a marker for trending. Inflammation is hugely pro-aging.
Bicep
#579
The book is “The Clot Thickens” and I highly recommend it. It’s an easy and entertaining read with no wading required.
The quote you asked after was actually quoted in the book and it came directly from the first paper I referred to above. The doubling of CVD risk for every 10 g/L I think came from the 3rd paper.
I was just wondering since my levels are so high already, would something bad happen if I increase it? It may decrease my CVD risk but increase my risk of something else terrible.
This is Ivor interviewing Malcolm:
MAC
#580
I love Malcolm, follow his blog. He’s anti-establishment re CVD.
You call 41-43 albumin level high?
Where I am, lab range is 35-52, so your albumin is nowhere near high. No doctor will pay any attention to a singular marker within lab range.
What is the objective of running your dosing experiment? You won’t learn anything about CVD risk for sometime, all certainly not all cause mortality.
Have a look though the studies and find the high dose range re your safety experiment.
If you believe it helps with inflammation, then maybe do before/after inflammation markers?
What’s your current hsCRP? Lipid markers good?
Bicep
#581
Yes, thanks for finding that for me. I like Michael, though his numbers would improve if he could get more people. n=1 doesn’t mean much and he spends half the video on it. Still since my average is around 42, and his graph looks like optimal is more like 49 this encourages me to increase my dose and see what happens.
As an aside, I was taking these:
Just one a day and never bothered to look at the label since I had no guidance at all of how much to take. It turns out the serving size is 5 pills and they are about as big as Mg Citrate. I’ll have to get a new pill sorter since this one is already completely full and my wife thinks I’m crazy already. This won’t help. Lol.
2 Likes
Bicep
#582
CRP is less than one. Lipids are high…LDL 150 at last check and HDL was 73. A year ago though my Lp(a) was very low. I only check that yearly.
I’m increasing my dosage of the Glucosamine, Chondroitin sulfate,MSM etc. Just to see what happens.
It’s a good thing our bodies run on automatic, I make so many mistakes, you know if it was important I think I’d be dead.
2 Likes
MAC
#583
Too funny, my sorter is borderline full too, and our wives share similar sentiment!
TG, Total Cholesterol?
Age?
Had a coronary calcium CT scan?
1 Like
MAC
#584
Went back to check (Feb '22), last Albumin was 48. I don’t normally add this marker to the panel.
Lp(a) is genetically determined I thought, so once you have gotten it checked once or twice, the levels will stay the same throughout your life.
I have high Lp(a) ( I am 24 and mine is 169) and unfortunately I have to wait until new therapies come out as PCSK9 Inhibitors arent usually covered by insurances unless you try multiple statins. Luckily there is the ASO clinical trials going on that gives me hope
1 Like
Yes Lp(a) is mostly genetically determined, and even PCSK9 inhibitors only lower it an average of 15% or so, at least according to a recent podcast (Peter Attia maybe?). I’m currently waiting for updated Lp(a) after going off amla and then going back on, to see if it lowered to any significant extent (acting as my own unblinded control n=1 experiment).
1 Like
tongMD
#587
There are potential natural PCSK9 inhibitors out there btw.
May be possible to get it from diet with a large enough effect without spending 10k per year out of pocket on expensive antibodies, assuming you’re throwing multiple darts hoping one or more actually hits. Another option is clinical trials using RNA targeting or gene therapy.
Can you let me know how that goes? I got some amla but I am waiting until I see my cardiologist next month to talk about plans
1 Like

")
