Bicep
#83
I use bulk supplement glycine. It comes in a 1 kg bag. NAC is hard to find since Amazon banned it, but you can just google. There is a bunch out there still. It’s a generic thing.
I’m not sure what to make of NAC, especially at the large doses. A friend of mine said that it greatly exacerbated his asthma. It gave me heart palpitations. I’m just taking the glycine. Seems safer.
1 Like
Rivasp12: if I’m recalling correctly, I believe the research done on the potential cardiovascular benefits of pine bark specifically used Pycnogenol (French maritime pine bark). The Bulk Supplements pine bark powder appears to be from a different tree species.
2 Likes
Nice pick up Brandy!
I didn’t think that there was a significant difference, but there well may be so I’m switching.
I found this French Maritime pine bark by Zazzee on Amazon. It’s 19.95 for #180 at 350 mg’s each.
Looks legit
More and more it’s being recognized that aging itself is a modifiable cardiovascular risk factor.
2 Likes
Bicep
#88
Talking about the 45000 MK4. Chris Masterjohn says the fat soluable vitamins are all broken down by the same biochemical machinery if unused. Taking one of the fat soluables in massive doses will rev up the machinery and this will cause deficiencies in all the others. He says to take them in proportion and if you increase one, you increase them all. He says 1000 is top for K2 and above that it’s a drug. At 1000 increase your A,D,E.
Just reporting what he says. He’s smarter than me. I just read it last night.
Thanks. That’s good information.
I don’t take it everyday, maybe 3 times per week.
Get plenty of A from diet and D from sun.
We thought this drug was going to be a miracle the way it lowered LDL and jacked up HDL. Not quite. No effect on mortality rates. Oops. Not that simple.
1 Like
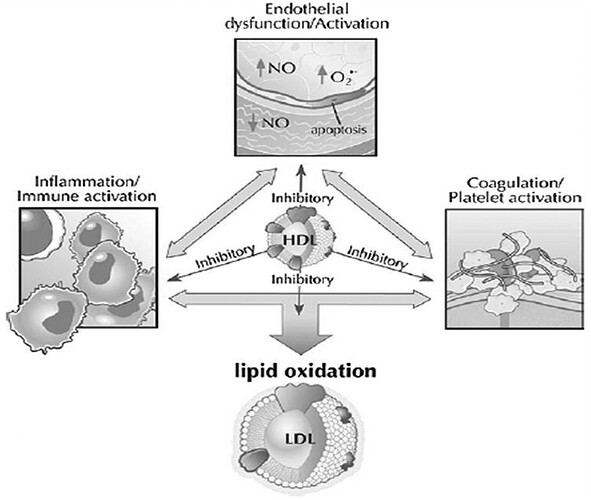
The whole hypothesis that HDL cholesterol is clinically relevant, in my mind at least, has been debunked for years now, given the failure of niacin and CETP inhibitors. Just shifting some cholesterol from LDL to HDL, though, doesn’t seem to me that it would be important. An LDL particle carrying slightly less cholesterol is likely just as atherogenic. Only meds that lower LDL particles are going to be clinically relevant it would seem, at least when it comes to lipid-specific, non-inflammatory mechanisms. On one of Attia’s podcasts with Tom Dayspring (lipidologist) they kind of make fun of the HDL hypothesis, as it’s been portrayed as some sort of molecule that floats around vacuuming up arterial plaques (hint: it isn’t).
2 Likes
I’m still studying and learning on this issue of LDL, HDL, APO-B, etc.
But yes - on the HDL issue the consensus now seems to be its basically irrelevant. I listened to this podcast with UCSF cardiologist Ethan Weiss and his focus really is on APO-B as the best predictor it seems.
1 Like
I quit taking Natto because of this paper. I wish it did work but this study in humans, larger than most, seems to refute the idea that it has any effect on CVD.
2 Likes
I remember way back when Framingham was all the rage and total cholesterol over 200 was the kiss of cardiac death. We pushed that Questran drug . And then came the statins . But myopathy, liver problems and memory issues kept us looking.
Then we had the good HDL which went up with exercise and alcohol. We were told that it couldn’t be high enough just like LDL couldn’t be low enough. And then HDL raising drugs had no, or even negative effects on mortality. Multiple population studies showed an inverse relationship with LDL levels and total mortality.
Now HDL is apparently a laughing stock and triglyceride/ HdL is yesterday’s news.
On to Apo B.
Of course, none of that has anything to do with whether we should outsmart our friendly longevity drug, rapamycin, by trying to negate its modest effects on lipids. I still have some serious reservations about that move, even considering Apo B.
5 Likes
Wouldn’t totally discard HDL just yet, especially as it relates to triglycerides. The ratio cutoff of 2.3 seems fairly predictive:
1 Like
I know this was meant this light-heartedly, but I still think it’s important not to anthropomorphize rapamycin or to characterize it as something with a pre-ordained purpose to make us healthier/younger. Idealizing it as such can create a bias towards overblowing the positives and downplaying any potential negatives.
5 Likes
We’ll, we’re taking meds for the lipids, meds for the glucose, and meds for the infections.
Wouldn’t worry too much about downplaying the negatives.
If anything we tend to forget that in multiple studies it prevents all age- related diseases. All. And there’s no convincing evidence to the contrary.
I’m also well aware that the evidence may change and then of course I’ll change my mind accordingly.
3 Likes
Bicep
#98
Drgathard,
Thanks for the paper. That is depressing. I’ve been taking the wrong pine bark and nattokinase, lol. Glad I found this site.
2 Likes
Given my high APO-B levels, I’m doing lots of learning on cardiovascular disease / atherosclerosis. Currently listening to these two podcasts, which seem pretty good (I’m a member of the Peter Attia website so have access to the full AMA podcasts, and recommend them).
and
2 Likes
Thanks for posting these very informative podcasts RapAdmin. Nothing in medicine is black and white and we must accept that there is much that we don’t know and the field is ever evolving.
There are studies which show the importance of apoB as an add on to the general lipid panel.
There are other studies that indicate that the apoB/ ApoA-1 ratio is the best indicator.
Still others that show no real value of adding apoB to conventional lipid assessments
I’ll now give several scenarios using myself as an example:
-
I’m 35 years old with no other risk factors but an elevated apoB level. You could argue that over 30 years I could develop atherosclerosis and should commit myself to a lifetime of lipid lowering drugs.
You could also argue that risks are additive, follow a good diet and exercise program, and follow coronary calcium scores while skipping the meds- at least for now.
-
I’m 67 years old, my calcium score is zero, but my apoB is high. You could argue that the chances are low that I’ll have a cardiac event before reaching the mean lifespan. But, let’s say that I intend to live to 100+ years, then you might be able to argue for lipid lowering meds.
But All meds have side effects so it’s not an easy decision especially if there’s no other risks.
This is complicated, difficult, grey, and depends on multiple factors.
I mentioned that I really like the pine bark and gotu kola studies. I also really like Amla extract as mentioned by Davin. It lowers TG, and the apoB/apoA-1 ratio. No effect on CoQ10. No apparent side effects.
Might be a good and safe compromise
4 Likes
José
#101
Attached are pages 37 to 40
rivasp12, Thank you for the information.
pages 37 to 40 (1).pdf (7.0 MB)
1 Like



")




