Yes, but AFAIK the lower doses had no identified hazard.
I am with you on pantethine. Just keep an eye out for bruising.
1 Like
zazim
#1995
Yes, likely safe although the failed outcome in the high dose study despite significantly reducing LDL and ApoB gives one pause. Even the red bean supplement isn’t bad for everyone. It is only toxic for people like me who are hyper absorbers.
I think you are right about that. A question for any molecule is how much is too much.
1 Like
scta123
#1997
You mean Red Yeast Rice? And why is bad for hyper absorbers?
zazim
#1998
Yes, that’s the one. There’s some discussion here around 30 minute mark. But a better discussion in another video that I can’t recall.
1 Like
zazim
#1999
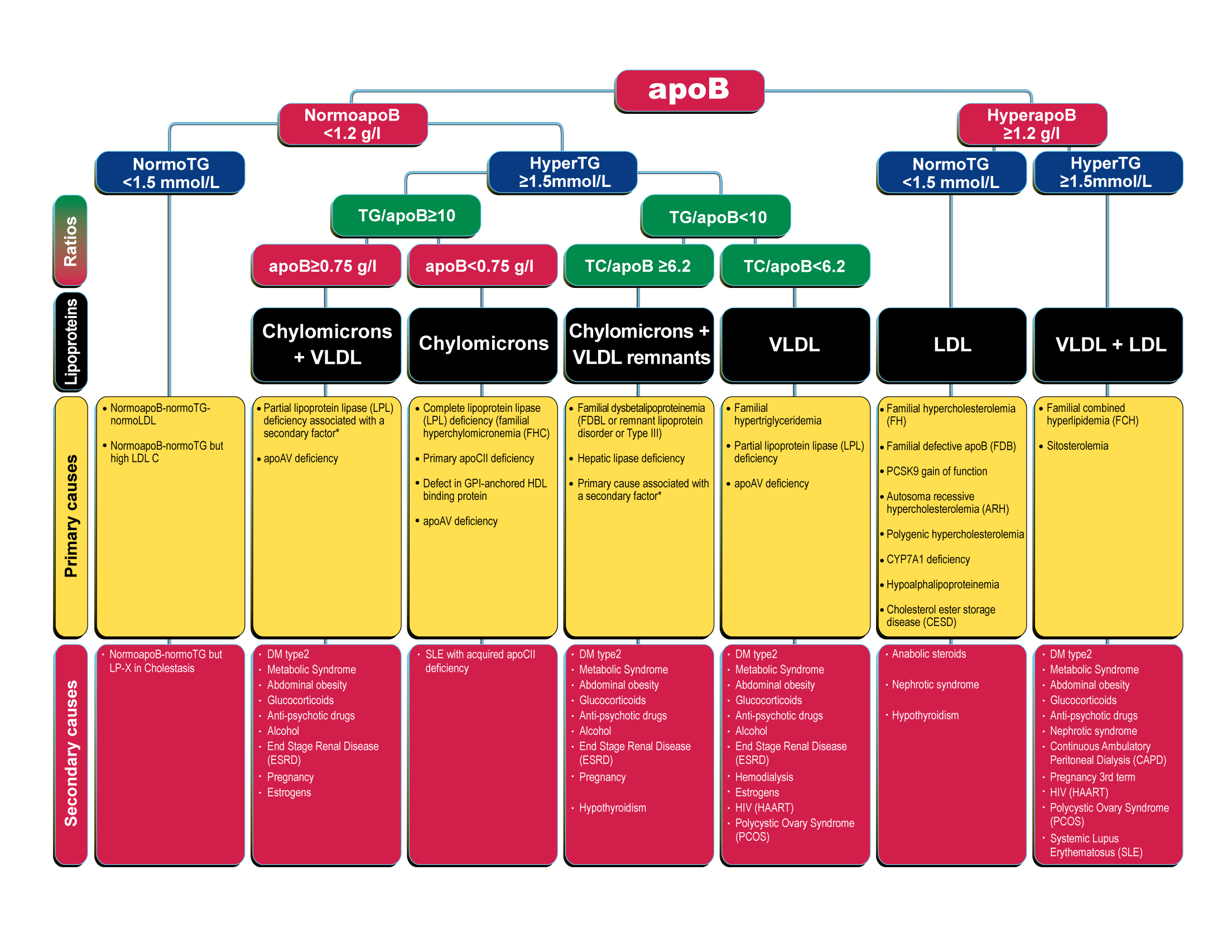
Here is a wonderful ApoB risk calculator from Alan Sniderman. It is especially useful if you have a discordance in your lipid results. This will focus the discussion with my primary physician.
https://apob.app/
Here is the algorithm.
1 Like
zazim
#2000
One more data point for some of the earlier discussion. I am on the far right side of the picture above so high risk for CVD.
My triglyceride to HDL ratio is .61. That is excellent, no matter how you measure it. My LDL-C is only mildly elevated at 109. But my risk is high. A CAC of zero wouldn’t change my risk profile.
1 Like
scta123
#2001
I think they were talking about another supplement, phytostetols, that might be helpful if you are not hyper absorber.
Btw tried this appB app you shared and did get similar result to what cardiologist’s assessment was. Even though I have apoB, LDL-C and TC that are borderline elevated and @AnUser insists I need to reconsider my and my doctor’s blindness in my risk assessment (which was low and lifetime risk is below 20% for ASCVD) I got this recommendation:
statin therapy might be given and this would be inappropriate. Even if pharmacological therapy is not initiated, raising concern as to whether a major risk factor is present is also inappropriate and could be psychologically harmful.
scta123
#2002
I recently was reading a study and some other texts by Sotirios Tsimikas, MD, who has a different view and suggests that niacin concurrent therapy with statins attenuates some of the possible unwanted effects of statins on atherosclerosis (they might rise Lp(a) and produce more Oxidized Phospholipids and while making concentrations of apoB lower they male them more atherogenic).
A_User
#2003
So it’s psychologically harmful to lower your ASCVD risk from <20% to much lower?
It’s more like your doctor is okay with that risk, which is weird.
It’s completely illogical.
2 Likes
zazim
#2004
Yes, I think you’re right on the supplement discussed there. There are no positive studies for niacin. It does lower cholesterol, but there are no positive studies.
scta123
#2005
I must say I never looked in depth of Niacin. I just remembered that it was mentioned as a possible concurrent therapy with statins. But it was a study from 2007 or 2006 and since probably there has been more in depth research on Niacin. Though there is also no financial interest in Niacin…
scta123
#2006
Completely illogical is that someone without medical training relaying on some you tube blogger(s) and his own very limited medical knowledge thinks he knows better.
There is no known medical intervention that would be advisable for low risk prevention of ASCVD other than lifestyle.
Assessment risk is a complex process. Borrowing you words, if 99% of 99 years old have advanced ASCVD in that case my risk assessment shows 80% reduction. Statins would possibly reduce it by few percents, but I and my doctor seem to be ok with taking this risk ATM.
And if taking statins without a proper assessment is a good strategy for yourself, go ahead. But if you think that taking statins will make your lifetime risk 0% I would have to say that on my current understanding and knowledge about ASCVD that you are delusional. If my fist sentence does not cover it already.
3 Likes
You can see here that a large percentage of people have an innate resilience to CAD despite very high LDL numbers.
https://www.ahajournals.org/doi/10.1161/circ.146.suppl_1.13515
It’s comforting to try to over simplify a very complex process involving not just lipids but a whole slew of other factors including even gum disease, inflammation, sleep, and even vitamin d status, not to mention the usual coronary risk factors.
As an aside, I’ve gotten a good reduction in LDL from citrus bergamot at 1000 mg and a friend reduced his ApoB by 26% on 1500 mg. No side effects.
3 Likes
A_User
#2008
Okay you don’t believe that reducing your apoB to 30-40 from 88 will reduce your risk for ASCVD by such a degree that the benefits outweighs the risks, I get it. Despite the fact that studies show a clinically significant reduction in MI’s in the short term, you can’t extrapolate in the long-term, for you. For some of us we don’t believe we have any risk from certain meds, at least if they don’t appear shortly after starting them - muscle pains, liver problems, etc. That means we have an unlimited upside and no downside. If you think PCSK9 inhibitors are near-risk free, maybe you believe it’s worth betting on that the reduction in ASCVD will be worth the cost. That’s up to you.
Also Thomas Dayspring says ASCVD cannot develop at physiologic apoB levels, lp(a) aside. So it’s not like something I’ve only taken from Peter Attia.
1 Like
A_User
#2009
Why do you keep linking observational studies?
1 Like
zazim
#2010
I take niacin to prevent kidney stones.
1 Like
Bicep
#2011
I like hearing all ideas, especially from professionals. I don’t see the harm. Much work went into the study.
You’re waaay to smart to fall for it though. You should call each of the people that did this study and explain to them that they’re wasting their time.
1 Like
On the Attia podcast with Dayspring, they discussed Niacin as a poor intervention for LDL. Dayspring said it required very large doses taken multiple times during the day. The rise in HDL is no longer considered important. Many other non-statin options to use before niacin for LDL. I take Niacin for NAD purposes, and because the flush makes me feel like I’m doing something important (I love a good placebo).
4 Likes