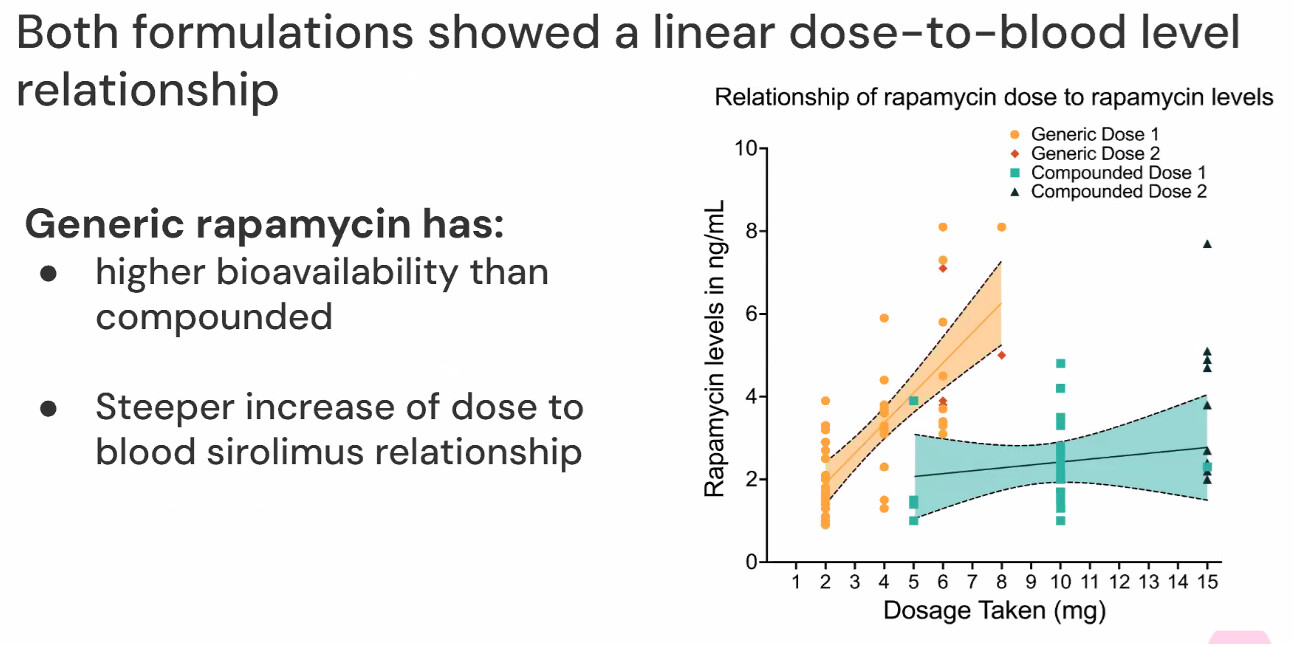
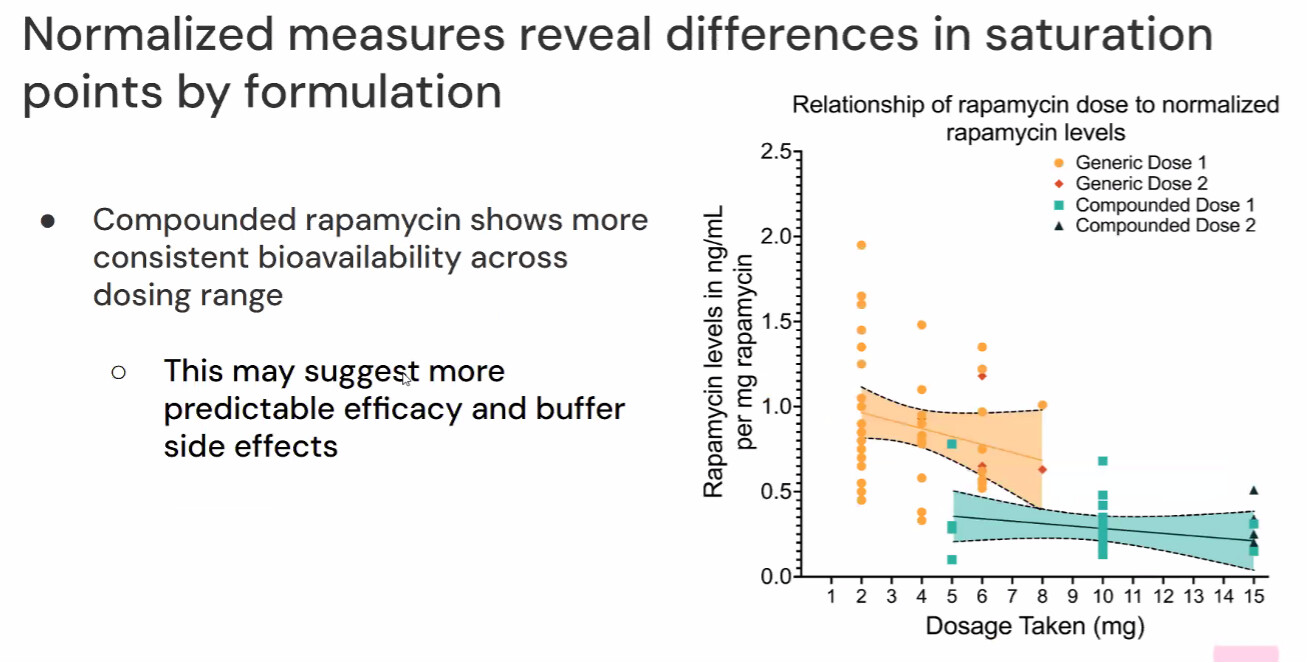
The PEARL study used tablets, prepared by their compounding pharmacy. (That was practically necessary to keep the study double-blind.) The PEARL team also used after-dose Sirolimus blood tests to study the bioavailability of compounded vs. branded/generic tablets. They presented results in a recent webinar. As this preprint paper says (lines 486-488) “we have discovered since the conclusion of this trial that compounded rapamycin is approximately 3.5x less bioavailable than commercially available formulations, suggesting that the 5mg and 10mg rapamycin groups received an average equivalent [of branded/generic Sirolimus] of 1.4mg and 2.9mg respectively.”
4 Likes
Bioavailability is not that simple – when the PEARL team analyzed Sirolimus blood levels 24 hours after dosing from multiple participants, they found significant variations among individuals taking the same dose (either compounded or generic), and they also found significant variations in the same individual taking the same dose on different dates.
5 Likes
I suspect that compounding pharmacies have a much lower consistensy and reproduceability production than FDA approved med company output. Personally, I’d rather minimize the odds of getting inconsistent product, and I’ll stick to industry products, thank you very much. This is not a knock on compounding pharmacies, there are some excellent ones out there, and a lot depends on a particular drug where some may be harder to consistently produce, just that I have no way of knowing any particular vendor, so it’s just a matter of minimizing possible risks. YMMV.
4 Likes
There is more to this bioavailability issue than the brief comment in the preprint that reports overall results of the PEARL study. I’d recommend reading the PEARL team’s bioavailability paper (https://www.medrxiv.org/content/10.1101/2024.08.12.24311432v1) before “rendering summary judgment”. For example see Figures 2 a, b, c and d in the paper. Here are Figures 2a and 2b from their webinar:
5 Likes
I dont think enough consideration is given to rapamycins mechaniam both for positive and negative effects. I think the peak concentration is more important for the positive effects than AUC.
5 Likes
pmoskie
#32
It would have been interesting to note what the patients ate prior to taking their dose since there is such variability within the same patient taking the same dose multiple times. Is there a gastric pH necessity? Is bioavailability affected by dairy products like erythromycins? Would be good to know this…
4 Likes
How does bodyweight affect outcomes?
Yes. If many participants lived in Florida and drank grapefruit juice daily, results could have been truly muddled. 
4 Likes
Zoom call discussing the new PEARL study is starting now - log in if you’re interested.
4 Likes
Do you have evidence of poor bioavailability with enteric coated capsules? I’d love a reference.
1 Like
WJ_PhD
#37
Interesting comment during the Q&A on how difficult/costly it would have been to match a true placebo to the unique shape of the rapamycin tablet.
2 Likes
This fits with my experience with Chinese powder compounded by me with lactose, at 1 mg per day, my trough levels were identical (3-4 tests) to “rapamune” brand capsules (which I had taken in the year prior). I recall that I was in the 2-4 ng/dl range (therapeutic levels 5-15 in transplant patients).
I have no idea if I am an outlier here. No grapefruit juice. Usually with high fat yogurt.
I now use enteric coated capsules but don’t test.
Jjazz
#39
The bioavailability difference could be driven by excipients in the capsules versus tablets. Even among tablets, we know that some brands have greater bioavailability than others. Zydus and Biocon, for example, have the predicted bioavailability, while Siroboon does not (at least based on anecdotal reports here).
Does anyone know where to find the inactive ingredient lists for each of these formulations? Do Zydus and Biocon include an excipient that is not present in Siroboon?
2 Likes
You can find the excipient lists on the tablets from all the major producers, but the capsules are from small compounding pharmacies, typically, so impossible to get data on them and their products. Siroboon also is a very small company, and impossible to get data on, from my searching.
1 Like
Jojje
#41
Did they have any goodies on the zoom call? 
LukeMV
#42
Is there a replay of the zoom call?
Also to note, these are self-reported periods which can have some variation. I participated in the bioavailability trial. I normally had taken the weekly dose on Saturday night, but moved it to Sunday night so that I could have a blood draw on Monday morning about 9-10 hours later. The level of accuracy of timing between the dose and the blood draw could not be expected to be the same as if both were in a clinically controlled environment. This has a high probability of impacting variability both individually and between individuals.
2 Likes
PEARL trial results webinar:
I haven’t watched it yet, so have no spoilers or spanners yet.
5 Likes
The apparent sex/gender effect is interesting. Two non-mutually-exclusive hypotheses:
-Women have lower body mass and a higher % body fat, (e.g. In this study,, men aged 50-60 weighed 88.2 kg and were 31.3% body fat, vs. 70.2 kg and 40% BF in women). So the same 10 mg dose would lead to substantially higher overall and lean tissue exposure for the women.
-Perhaps females benefit more from rapa, as in the mouse studies (though this itself seems to be at least in part due to blood levels)
1 Like