Neo
#22
Of course. Just trying to share some issues that I saw in the logic. No need to discuss further.
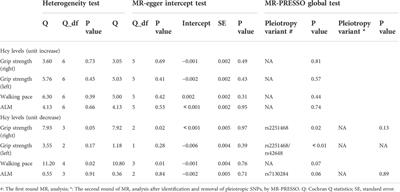
Look at the Mendelian randomization studies. Genetically high homocysteine is different than homocysteine from other causes, and directly reducing homocysteine via betaine may not have the effect as going after the more upstream factors (some which are really tough)
B vitamins don’t reduce my homocysteine, which is sad. But maybe I can try betaine and see how it goes
2 Likes
adssx
#24
What do you mean? I posted many MR studies here:
The MR study you posted isn’t great btw (2 citations, unknown authors, tier 2 Chinese uni, low-quality journal).
1 Like
Is there a difference between Active folate (5-MTHF
adssx
#27
Update on this:
- My homocysteine was indeed quite high: 18.1 µmol/L

- My folic acid was normal (7.7 µg/L), while my vitamin B12 was suboptimal (302 pg/mL, vs > 600 for optimal).
- So, I started methylcobalamin 1,000 µg daily (sublingual).
- Retested after 2 weeks: homocysteine lowered to 12.2 µmol/L (–33%), and B12 increased to 426 pg/mL (+41%).
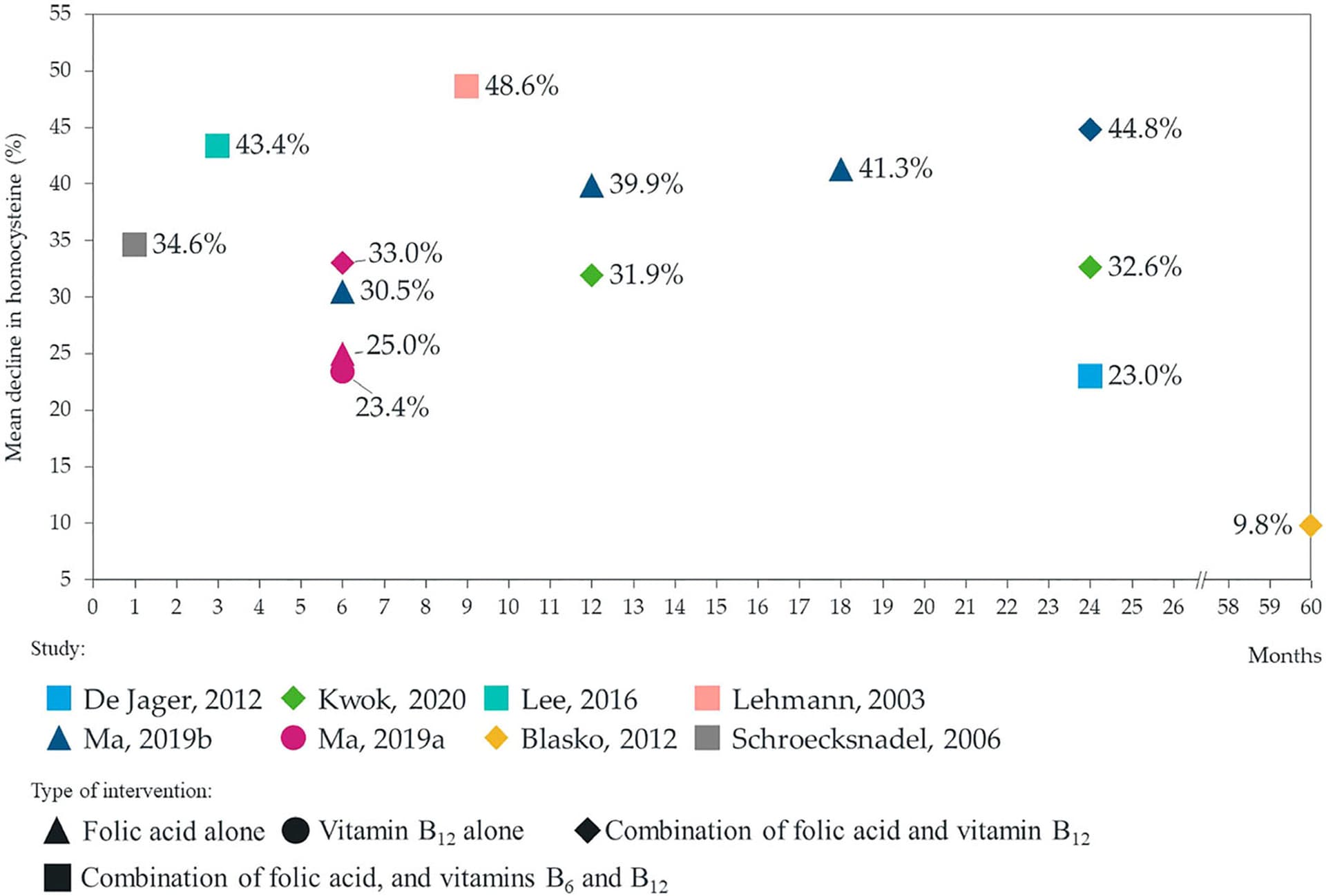
This is in line with the literature that reports ~30% reduction in homocysteine levels after B9 and/or B6 and/or B12 supplementation: Impact of supplementation with vitamins B6, B12, and/or folic acid on the reduction of homocysteine levels in patients with mild cognitive impairment: A systematic review 2021
I didn’t expect to see results in just 2 weeks. It seems that it takes 12 weeks to get the full effect of B12 supplementation on homocysteine levels: A comprehensive review and meta-regression analysis of randomized controlled trials examining the impact of vitamin B12 supplementation on homocysteine levels 2023
I’ll keep supplementing with methyl-B12 to reach ~600 pg/mL. I’ll measure homocysteine again, as I’m curious, but based on what I posted a few weeks ago, I don’t think it matters.
2 Likes
Neo
#28
Do you know your B6 levels? In case deficient or low in that might want to consider upping that a bit in diet or supplements too.
What are you basing the target of
-B12 to reach ~600 pg/mL
on?
A_User
#29
You should probably measure methylmalonic acid too: How to Test for Functional Vitamin B12 Deficiency (video/transcript).
Cyanocobalamin is probably better than methylcobalamin: Coenzyme Supplements: Methylcobalamin and Adenosylcobalamin – Vegan Health
1 Like
adssx
#30
No, unfortunately, it’s not offered by the various labs I use. Also, I preferred to go step by step, one intervention after another, to clearly identify the impact. (On top of that, see below, B12 but not B6 might be neuroprotective.)
- The lab gave that as the “optimal” range (vs “normal”).
- My “longevity” doctor said the same.
-
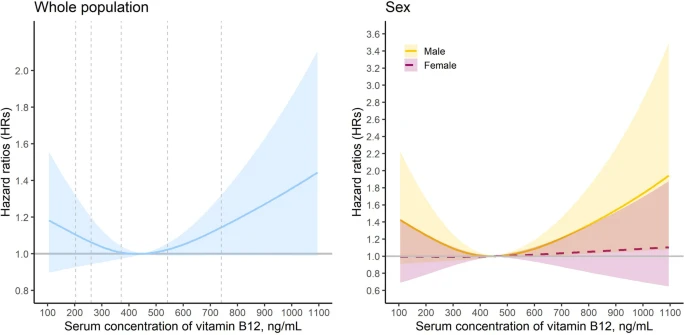
LifeExtension says: “While the normal range is generally 160–950 picograms/mL (or 118–701 picomoles/L), a B12 level of at least 540 picograms/mL (400 picomoles/L) is needed to keep homocysteine levels from rising. The combination of a B12 level in the lower half of the normal range plus an elevated homocysteine level is indicative of metabolic B12 deficiency.” They cite Cardioembolic stroke: everything has changed 2018. However, after checking other sources, it’s really fuzz: “A linear trend dose-response analysis showed that each 100 pmol/L increase in serum vitamin B12 concentration was associated with a 4 % higher risk of all-cause mortality in the general population (adjusted HR 1.04, 95 % confidence interval CI 1.01 to 1.08; n = 8; P non-linearity = 0.11) and a 6 % higher risk for all-cause mortality in older adults (adjusted HR 1.06, 95 % CI 1.01 to 1.13; n = 4; P non-linearity = 0.78). […] The meta-analysis of cohort studies showed a positive association between a high serum vitamin B12 concentration (>600 pmol/L) and all-cause mortality (adjusted HR 1.50, 95 % CI 1.29 to 1.74; n = 10; p < 0.01) […] Similarly, serum vitamin B12 concentrations (400–600 pmol/L) were associated with increased all-cause mortality (adjusted HR 1.34, 95 % CI 1.10 to 1.64; n = 9; p < 0.01).” (The origin of vitamin B12 levels and risk of all-cause, cardiovascular and cancer specific mortality: A systematic review and dose-response meta-analysis 2024) Please note that 400 pmol/L = 540 pg/mL and 600 pmol/L = 813 pg/mL. This Chinese paper found a reference value for vitamin B12 of 450 pg/mL (332 pmol/L, I think they got the unit wrong in their charts):
While another paper found the opposite: “In the general population of NHANES, low serum B12 concentrations were associated with a moderate increase in all-cause mortality.” (Relationship between serum B12 concentrations and mortality: experience in NHANES 2020)
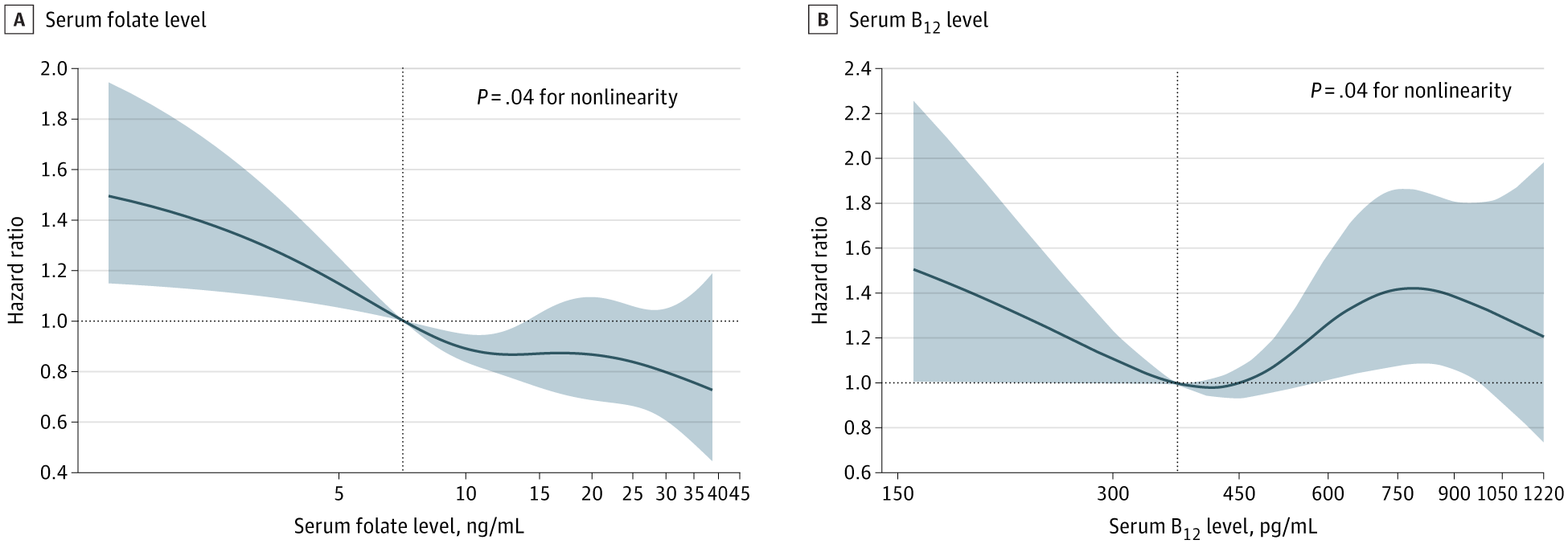
See also: Associations of Serum Folate and Vitamin B12 Levels With Cardiovascular Disease Mortality Among Patients With Type 2 Diabetes 2022: “This cohort study found that both low and high serum levels of vitamin B12 as well as low serum levels of folate were significantly associated with higher risk of CVD mortality among individuals with T2D.”
(optimal at ~400 pg/mL = 300 pmol/L?)
Also, methyl-B12 might be neuroprotective, which was another reason for me to increase my low-ish levels:
So I guess based on all the above I’ll keep supplementing with methyl-B12 without going above 600 pg/mL?
adssx
#31
I think it’s the opposite. That’s why Attia and “Dr Lipid” are taking methylcobalamin and not cyanocobalamin. Methyl-B12 does not harm the kidneys and might be more effective. See also:
Also, methylcobalamin, and not cyanocobalamin, seems neuroprotective.
A_User
#32
With renal failure, yes. I think it is unlikely harmful for kidneys with those with normal function, and my comment were relating to treating vitamin B12 deficiency. I use it since it has a track record and is stable, and consequences of vitamin B12 deficiency is not good - might optimize with other forms later.
adssx
#33
Kidney function starts declining at age 30. If it’s bad for people with renal failure, then I think it’s safe to assume it might be bad for kidneys in general if you use it over the long run. Is there any risk of using methylcobalamin instead of cyanocobalamin? If not then I see no reason not to use methylcobalamin.
2 Likes
Neo
#34
Thanks, helpful stuff.
A few comments
Getting the data for B6 does not mean that you have to supplement with B6 at the same time as B12 though, but rather that it will make you understand the B12 & Homocysteine data better as it is in context of the B6 (similarly to how have the B9 data).
Frustrating and weird that it’s tough to get a B6 test.
Seems like each of those are associations/correlations?
What drives the correlations? As one plausible example, could it be that cancer and all cause mortality is higher in (a) heavy meat eaters than in (b) vegetarians, pescatarians and vegans (also based on general health consciousness/behaviors of groups (a) and (b) on average, not just because heavy (processed) meat consumption could drive cancer). If so the association between B12 and cancer is not because of B12 being causal but because other things in the heavy meat eating group, (a), are causal.
Have you seen causal or mechanistic reasons for why B12 would drive cancer?
1 Like
Do we have animal studies on injecting high dose vitamin b12 directly into the bloodstream?
adssx
#36
Of course, it’s just that given the lack of availability of B6 tests in labs I use, I didn’t bother more.
Yes. I don’t know what the mechanisms could be, but there are ongoing studies of methyl-B12 for PD and ALS, we’ll soon know.
adssx
#37
This paper offers some answers (or at least eliminates some potential mechanisms): Are serum concentrations of vitamin B-12 causally related to cardiometabolic risk factors and disease? A Mendelian randomization study 2018
We found no evidence for a strong causal relation between vitamin B-12 and BMI, waist-to-hip ratio, serum leptin concentrations, body fat, fasting insulin, HOMA-IR, glycated hemoglobin, CAD, T2D, or HDL, LDL, or total cholesterol. This implies that increasing serum concentrations of vitamin B-12 through dietary changes in vitamin supplementation is unlikely to have major effects on these traits. Our results suggest that previously reported associations between vitamin B-12 and cardiometabolic traits from observational studies may be a product of bias, confounding, or chance. However, we did find some evidence for a causal effect of vitamin B-12 on fasting glucose and HOMA-B in normoglycemic individuals. The causal relation between vitamin B-12 and fasting glucose and HOMA-B should be replicated and further tested in a population that includes hyperglycemic individuals before final conclusions are drawn.
2 Likes
Neo
#38
Are those studies to lower or increase B12?
adssx
#39
1 Like
Neo
#40
Thx @adssx so in totality it seems like we don’t have to be too worried about the mortality associations at this point?
adssx
#41
I think so, and that’s my current bet. But it’s not super clear either, as, per the above BMJ article: “there is no “gold standard” test to define deficiency” and “Measuring serum biomarkers such as B12 or methylmalonic acid is neither helpful nor indicated in assessing or monitoring clinical improvement, neither is titration of injection frequency based on biomarker assessment”
1 Like