SNK
#21
no my BMI is only 34 LOL. Kidding most likely around 25-26 ish.
1 Like
Thorin
#22
At this time the drugs are not ‘indicated’ for you. The “on-label” requires type 2 diabetes or a BMI >30 or a BMI > 27.5 with at least one other weight related issue (high blood pressure, dyslipidemia, …). Of course an MD could prescribe these for you off-label.
Anyway we don’t have a lot of data for people in your category. Absent some compelling data, it does not seem like an intelligent risk:reward choice for you to take these drugs. Also they are not cheap.
Most medicine needs to be individualized to the patient. I guess there are a few exceptions (such as certain childhood vaccines), but generally speaking, standardized treatments are bad medicine.
2 Likes
Regeneron founder issues warning on GLP-1 Drugs.
Davin8r
#25
Non-paywalled version (for me, at least):
He’s not unbiased, since Regeneron is working on muscle building drugs (myostatin inhibitors).
1 Like
adssx
#26
Pay walled for me: what is his reasoning?
Here’s the content of the article
The co-founder of biotech firm Regeneron Pharmaceuticals (NASDAQ:REGN) said in a newspaper interview that popular weight-loss drugs could be harmful to people who lose too much muscle mass that’s seen as helpful in keeping the weight off. His company is currently testing medicines to preserve muscle mass.
The weight-loss drugs known as GLP-1s have been shown in clinical studies to cause muscle loss that exceeds what people lose when they try shedding pounds through diet or exercise.
This muscle loss adds “insult to injury” for patients who discontinue GLP-1s and gain back weight, George Yancopoulos, who also is Regeneron’s (REGN) chief scientific officer, higher body fat percentage that’s associated with other health problems, he said.
Drug Trials
Regeneron (REGN) isn’t alone in researching experimental treatments for preserving lean muscle mass when combined with GLP-1 drugs that curb appetite. If the $130 billion market for GLP-1 drugs is any indication, there is ample demand for muscle-preserving treatments.
Novo Nordisk (NVO) (OTCPK:NONOF) currently markets Ozempic and Wegovy for weight loss, while Eli Lilly (NYSE:LLY) makes Mounjaro and Zepbound.
Regeneron (REGN) is testing a drug called trevogrumab that blocks the hormone myostatin, preventing from limiting muscle growth, in combination with Wegovy in mid-stage trials.
Meanwhile, there are 11 myostatin drugs in the industry pipeline, of which seven are being investigated for obesity, the FTI reported, citing data from industry tracker Citeline.
Eli Lilly (LLY) last year acquired Versanis for $1.9 billion to obtain a muscle-preserving treatment. Newly listed BioAge Labs (NASDAQ:BIOA) partnered with Eli Lilly (LLY) on a treatment to prevent muscle loss.
3 Likes
adssx
#28
Thanks. Ok so nothing new and the guy is just promoting his own company.
7 Likes
I just heard that this is the essential function of GLP-1 (representing about 1/2 of the “make more insulin” signal). A lot more insulin would help bring blood glucose down but what is happening with people who don’t have high blood sugar despite being overweight? They get higher insulin (via GLP-1) and then low blood sugar and then the pancreas puts out glucagon and then the liver puts out glucose? So everything gets up regulated? It sounds like the system is getting overclocked.
Am I understanding this right?
2 Likes
Beth
#32
Interesting that it shows ageless appears to have a liquid to place under one’s tongue
I have no problem with needles (it’s the only thing I’m not wimpy about!) but I am curious why most of us don’t seem to be using this or pills?
1 Like
Rob01
#33
As background I don’t have T2D, I traditionally have low fasting insulin less than 3.0 mcIU/ML and A1C between 5.1 and 5.4. I’m also 12% body fat and very active. 12% body fat was from a DEXA after 3 months on Triz.
In my experience since starting to experiment with Tirzepatide (4 mg / week) fasting insulin levels don’t change much and maybe go even a bit lower (last fasting insulin reading based on 3 months of TZ was 2.0 mcIU/ML) and A1C was 5.1%. I typically need either SGLT, Metformin or GLP1 to get an A1C of 5.1. Without any meds it will be like 5.4.
1 Like
These are junk, which is why relatively nobody uses them. The molecule is way too big to be orally absorbed effectively without help (such as SNAC technology found in branded oral semaglutide (Rybelsus), and even that doesn’t work very well).
The next GLP drug to be approved (early next year) is orforglipron, which is a “small molecule” and is orally bioavailable. It’s an agonist at GLP-1 and GIP (same mechanism as tirzepatide) and should be fairly revolutionary given the convenience factor of popping one pill daily. Eli Lilly just invested $550 million to stockpile the pills in preparation for its release.
8 Likes
I’d need to see area under the curve insulin levels in various populations to know if these meds actually increase average/total insulin levels over time. I’d think it also depends on the subject. For instance, I’ve lost about 25 pounds of fat from my midsection since being on a GLP, and I’m now very lean and cut. Certainly this has increased my insulin sensitivity such that my muscle and liver no longer need as much insulin in the first place, so does this cancel out the increased insulin stimulated by the GLP med over any given 24 hour period? Hopefully!  . Doing a fasted insulin level would be interesting, but it still wouldn’t capture the full picture. Ideally we’d have a CGM-type device that measures insulin. I hope that’s in the works!
. Doing a fasted insulin level would be interesting, but it still wouldn’t capture the full picture. Ideally we’d have a CGM-type device that measures insulin. I hope that’s in the works!
At this point it wouldn’t seem like a good idea for anyone who is already lean and metabolically optimized to use a GLP med, but then again why would they?
1 Like
LukeMV
#36
What a brutal name to try to pronounce for something that could become a blockbuster drug
4 Likes
Many of my friends are using oral Rybelsus and have been losing weight. My courier has lost 20 lbs in 2 months and said her snack cravings have disappeared. Her whole family is switching to the pills, which are much cheaper and easier than the injections.
I’m considering the pills as well since it’s a no-hassle intervention, even though the doses are larger due to ingestion. In the end, the same result is achieved without worrying about all the hassles and risks of injections. It’s a lot cheaper too!
2 Likes
man_li
#38
Can you share where to buy it? thanks.
You can buy them from Indian Rapamycin suppliers. I used Jagdish and Maulik. They both sell them.
How much is Rybelsus 3 mg 7 mg 14 mg oral?
Maulik:
35$ - 3 mg
39$ - 7 mg
43$ - 14 mg
For 10 tablets each
Jagdish:
1- RYBELSUS 3MG (SEMAGLUTIDE 3MG) = USD 45 Per 10 Tablets
2- RYBELSUS 7MG (SEMAGLUTIDE 7MG) = USD 50 Per 10 Tablets
3- RYBELSUS 14MG (SEMAGLUTIDE 14MG) = USD 55 Per 10 Tablets
It is expensive though. It will cost you about $160 USD a month. But probably worth it compared to other stuff we may buy that is not as effective.
4 Likes
man_li
#40
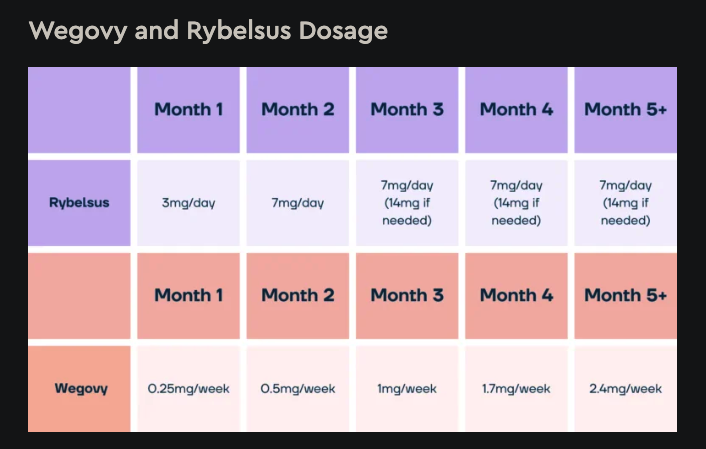
The dosage for treating diabetes in the instructions is to take one tablet (7mg or 14mg) per day.
I don’t have diabetes. To further reduce the cost, can I take one tablet (14mg) every few days(just like Wegovy/Ozempic injection)?
thanks.