Interesting paper. What I find odd is the absence of discussion about nutritional choices to allow our microbiomes to make the butyrate!
Absent fuel… probiotics get you nowhere… and are expensive.
I have major “issues”. Crohn’s disease, myasthenia gravis requiring a decade of high dose prednisone. Recently (and unsurprisingly), steroid induced type 2DM. I started Rapamycin not for it’s longevity but for it’s effect on Treg/Th17 balance (5-6 years ago)…
In my attempts to resolve the diabetes I have, of necessity, needed medications. That was insufficient. Ditto fairly extreme carb restriction (and exercise).
The missing piece for me was soluble fibre. In amounts few others approach.
Most days 75 g of soluble fibre. Some days in excess of 125g.
Unlike most who abandon acarbose because it provides “fuel” for fermenters, I embrace it!
Two days ago I consumed 75 g of non fibre starch with 125mg of acarbose… most of that never hit my bloodstream. Gas? Nope!
I have converted a dysbiotic leaky gut into a fermentation and scfa producing factory.
It has not been easy, but it is doable.
I’ll also weigh in on a paper posted elsewhere about inulin.
No surprise at all that a SINGLE DOSE of 30 g caused bloating, gas, colonic distension (and gut leak) in some, but not all subjects. My prediction is that they lacked the intestinal ecology to handle this huge dose in terms of fermentation, different other dietary choices that exacerbated rapid early fermentation and no secondary gas metabolizers.
I just finished my usual breakfast of 200 ml of yogurt, 12 g each of creatinine, psyllium, inulin and potato starch. There will be zero gas, distension or distress.
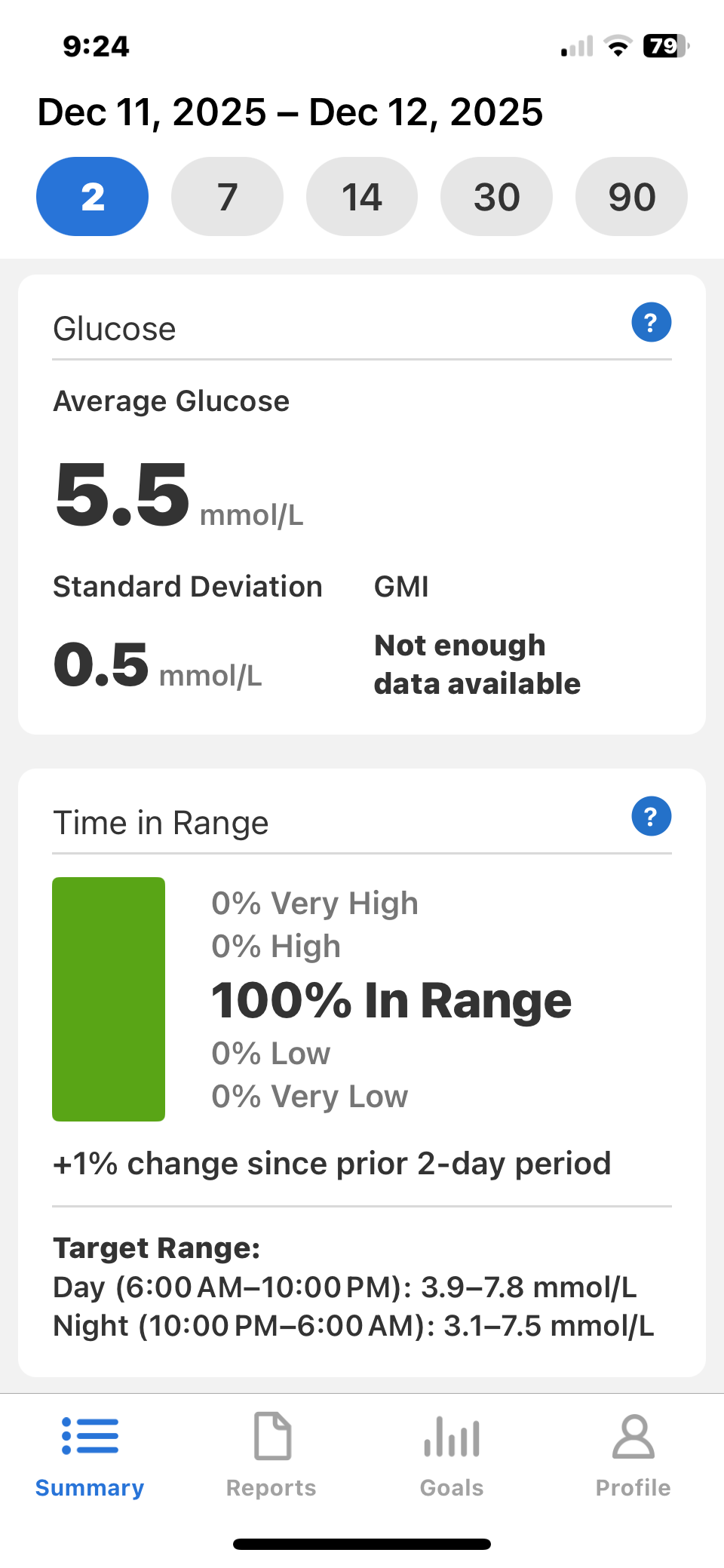
How is it working?
I’ll try to add a clarity screenshot.
Remember, this is a guy on 15-50 mg of prednisone for a decade!
BTW, my dexa… 12.8% fat, and a T score (not Z score), of 1.5! No sarcopenia.
My high order conceptual model has had major upgrades, and I think its working.