Eades wrote a bit on calcium scans and atherosclerosis this week. It’s fairly long as usual, but easy reading. I don’t know what to think. He says angiograms are not completely safe, do a stress echo instead. Interesting but not conclusive:
A physician reader emailed me an interesting story about his own calcium score, which I’ve copied below.
With all the talk recently about making more use of calcium scores, and in your newsletter, I have an unusual story as far as I can tell I think you would be interested in.
I have quite a family history of heart disease. Grandfather father and brother dying of heart attacks. Through the years I’ve tried to watch my lipids, of course following the [prevailing] theories of the time, didn’t eat eggs for 25 years, all the things that at one time we thought were gospel. I have taken statins for 30 years of one type or another.
Briefly, I developed atrial fibrillation and the cardiologist recommended having it converted. I woke up in my room with the cardiologist there and he said he had “good news and bad news”. He noted that on the first shock that my heart converted, but that the shock put me into “third degree heart block”, and he told me that I would need to have an emergency operation that night to place a pacemaker.
Two years later in 2018 I had some runs of un-sustained ventricular tachycardia, and an arteriogram revealed one obstruction in my coronary circulation in the LAD. This was stented.
Even though I had had a stent in the LAD and a pacemaker, I had never had a calcium score.
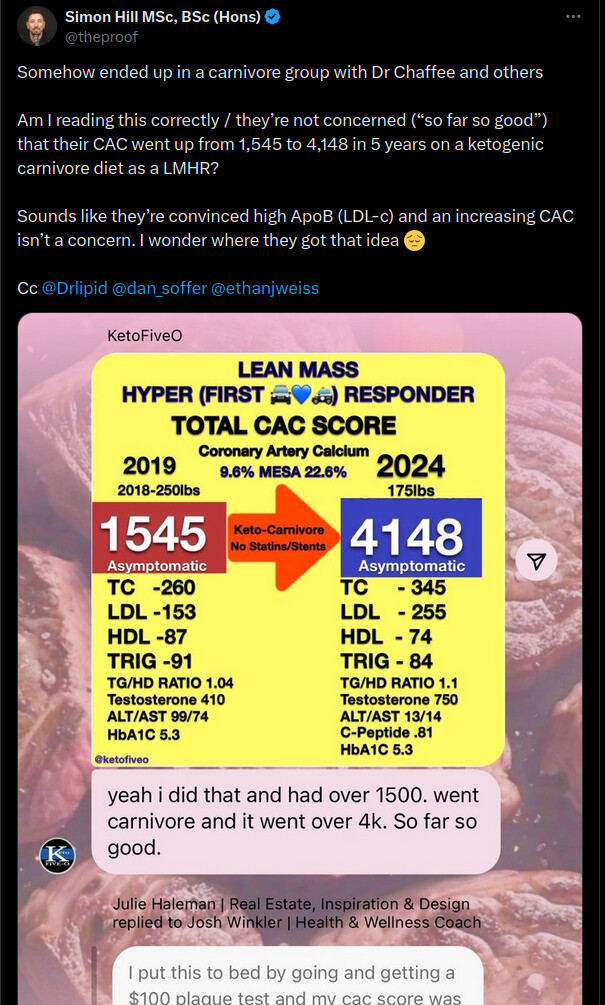
For the next five years I indulged heavily on everything scientific about metabolism and listen to all sides. After listening to Ivor Cummins and Peter Attia talk about the calcium score, I thought I would get one in March 2023. My score was 1300 and it was 99% all in the LAD. I freaked out.
I went back to the cardiologist who did the stent and he could see how upset I was and he said that he would do whatever was necessary to decipher the extent of my disease. So I said I wanted a coronary arteriogram. Here’s the kicker. The coronary arteriogram was 100% normal, no obstruction in any vessel. LAD 100% flow. Staggering!
Since I had been on statins for 30 years, my cardiologist hypothesized that the increase in calcium that is seen with long-term statins, so-called statin paradox, calcified my interstitial coronary artery, but the calcium moved to the periphery and it did not obstruct the vessel at all.
So I said to him I have a “hard pipe” with normal flow and he responded “exactly right”.
https://consultqd.clevelandclinic.org/plaque-paradox-statins-increase-calcium-in-coronary-atheromas-even-while-shrinking-them
I have listened to a lot of books and lectures, but I have not heard exactly anything like this. You may want to comment on this? [Link above in the original]
This man’s history is educational at multiple levels.
Many people conflate a high calcium score with heart disease. If you’ve got a high calcium score, then, supposedly, you’ve got serious heart disease. Which, as this man’s history shows, is not always true. A high calcium score and serious atherosclerosis does not always correlate.
Plaque can be protective. It usually forms at junctions in the coronary arteries where blood flow creates the most shear stress. [The Bride reminds me I was a civil engineer before I was a doctor, so considerations of sheer stress is in my DNA.] When blood is flowing along a straight pathway, flow is usually laminar, which means smooth and without turbulence. Coronary arteries are more serpentine than straight. When the arteries divides into two smaller arteries, or when it makes a sharp turn, the blood flows goes from being laminar to being turbulent.
You can hear this change even in a garden hose. Next time your watering something with the hose going full blast, bend the hose. If you listen, you’ll hear a hissing sound at the turn, which means the flow inside the hose has gone from laminar to turbulent.
If you were to take a hose, put multiple bends and kinks in it, then run water at high pressure through it 24/7 for a while you would find damage to the inside of the hose where all the kinks and turns are. But not in the parts that are straight.
It’s the same with coronary arteries. The turns, kinks, and bifurcations are where all the stress is.
Plaque develops to strengthen these areas analogous to patching a pot hole with asphalt. Since plaque contains around 20 percent calcium, the calcium shows up on a calcium scan. If you see a lot of calcium, then there is a lot of plaque. But the plaque may very well be protective and not pathological at all.
What causes heart attacks, if plaque is at the root, are bits of it breaking off and floating downstream until they end up blocking the flow of blood.
If you have a lot of plaque that ends up creating a narrowing, you may have chest pain if you over exert, but it usually goes away once the need for excess blood flow resolves. That process is called angina, which is pronounced differently all over the place. Some say ANgina whereas others say anGINa, not an-GEN-a, but an-GIN-a, with a long I. (Those of us who were taught how to say it properly in the South, say ANgina.)
One can have a lot of protective plaque and still not have heart disease as long as the lumen (the interior of the artery through which the blood flows) is open. If there is a canal the blood can travel along without obstruction, you shouldn’t have an issue.
Way back in 1964, Dr. George Mann (who was an associate director of the Framingham Heart Program) studied heart disease in the Masai in Africa and found it to be non-existent. He ran EKGs on 400 males with a handful of children and women included in the study. He found minimal abnormalities. He also looked at cholesterol levels in 388 Masai males and found only eight to have levels over 200 mg/dl.
The reason Mann was curious about the Masai is that members of this tribe consume huge quantities of milk and meat. When milk is scarce, they will open an artery on a cow, collect blood (not enough to kill the cow, which is a valuable commodity) and drink it. Mann’s work at the Framingham study sensitized him to the association between saturated fat intake, cholesterol levels, and heart disease.
Years later, Mann went back to Africa to take another look at the Masai and heart disease. This time he evaluated 50 autopsies of Masai who had died in accidents and other non-heart disease ways. He discovered that the Masai had extensive atherosclerosis. In other words, a lot of plaque. But at the same time, no occlusion; the openings in the arteries through which the blood courses were large.
We find the Masai vessels do show extensive atherosclerosis ; they show coronary intimal thickening which is equal to that seen in elderly Americans. The unique anatomical feature of the Masai material is that the coronary vessels enlarge with age so that the lumina are not compromised by intimal thickening.
I suspect this is exactly what happened in my respondent’s case: he had a lot of plaque, therefore a lot of calcium and a high calcium score. But at the same time, he had wide open arteries that had enlarged over time. He had great coronary blood flow, so no signs of heart disease despite a huge calcium score.
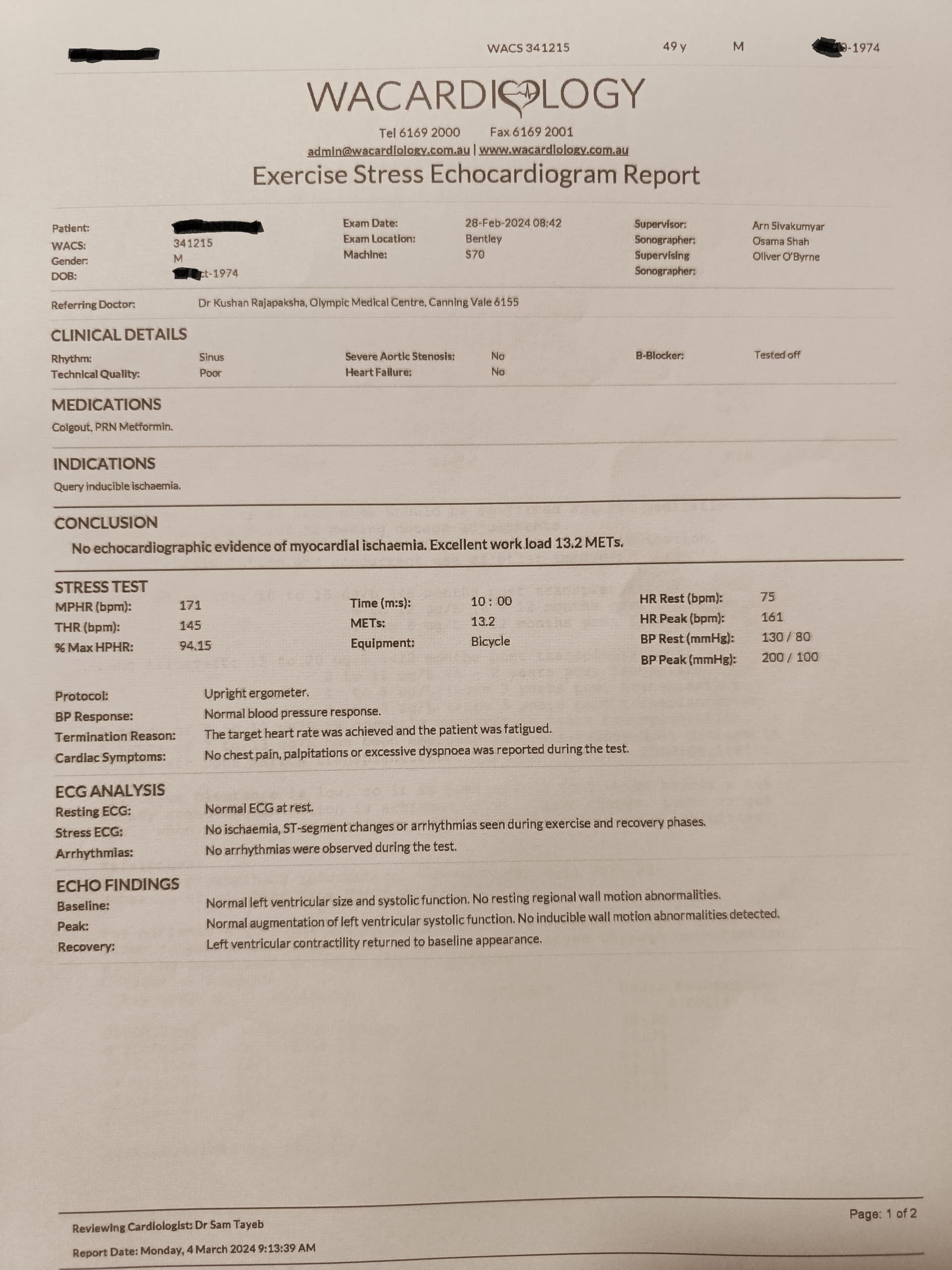
If you do get a calcium score that is high, don’t make a run to the cardiologist to get an angiogram. Angiograms are not necessarily benign procedures. Things can go wrong. Your best bet, in my opinion, would be to get a stress echocardiogram first. If that is normal, you’re probably in pretty good shape heart-wise. Of course, if based on what your cardiologist finds on the stress echo, something else is warranted, then by all means take the test. It’s been my experience that a normal stress echo makes everyone—cardiologist and patient—feel a lot better in the face of a high calcium score.
As to the article linked above in the quote, maybe statins do stabilize plaque. But I don’t think anyone knows for sure. There are fewer fatal and non-fatal heart attacks in those who take statins than there are in those who don’t. Maybe that’s a consequence of plaque stabilization. But, overall, the total death rate, or all-cause mortality—is the same in both groups.
I’ve seen that a low-carb diet will stabilize plaque as well. I’ve known patients who were agitated because they went low-carb after discovering an elevated calcium score only to re-take another test in a year or two and find a higher score.
Which is why I much prefer the method of risk calculation described in this paper I’ve discussed a few times in the past. It doesn’t rely on the calcium score you get when you get scanned, but on a density score that more accounts for the stable plaque.