A_User
#48
TMAO doesn’t cause heart disease, I don’t know about anything else.
1 Like
kansel
#49
You are right, I meant 2grams of each per day, sometimes I actually do 3 gram of each per day. The kidney stone thing might be the case for some, but never happened to me. But even kidney stones beat open heart surgery lol.
A_User
#51
Mendelian randomization studies show that TMAO doesn’t cause heart disease, another reason why to be skeptical of association studies for complex things. They often fail, in prestigious journals, and perfect quotes that can be cited on forums like this one.
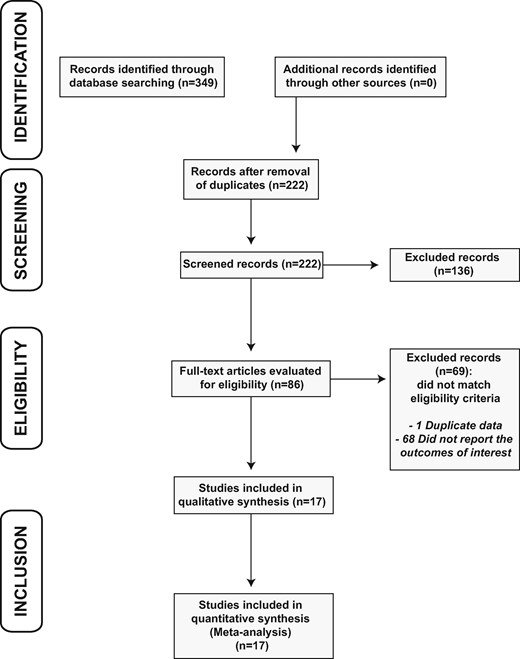
Overall, a high TMAO level was associated with both major adverse cardiovascular events (RR = 2.05; 95% CI 1.61–2.61) and all-cause mortality (RR = 3.42; 95% CI 2.27–5.15).
At first glance many people will believe that is real and the risk is as such. When there is no such thing in reality.
Can you share the study with the conclusion you describe? I’m interested in this topic.
This study used Mendelian randomization to show TMAO is causal for high BP https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9354484/
“Our study provides evidence of a causal relationship of TMAO and its precursors with BP, suggesting that mediating the generation of TMAO would be beneficial for lowering BP.”
1 Like
Thanks. This is interesting. I’ve reviewed a few other studies on TMAO, all of which support the hypothesis that TMAO leads to AGE/cross-linking which causes arterial stiffening which leads to higher BP and CVD. This study used mice to study adding TMAO to see the impact…they found TMAO is causal. I think it’s too early to conclude TMAO isn’t a problem.
https://www.ahajournals.org/doi/10.1161/HYPERTENSIONAHA.120.16895
3 Likes
First off, terrific conversation. I am very much enjoying the lively and constructive discourse on what can (at times) be a decisive topic. I had hesitated throwing the protein level “grenade” in the forum, but am ecstatic with the resulting discussion.
@Joseph_Lavelle : If you are interested in reducing arterial AGE-based cross linking (or any AGE in which serum/blood flow can reach), wouldn’t a supplement of carnosine (or beta-alanine as a precursor) be appropriate alongside reducing TMAO? I have read about risks with TMAO as well, and had come to the carnosine conclusion earlier in my quest to stave off the likely inevability of increased CVD risk from my (healthy) low-carb diet and exercise, but from polling the opinion of this forum I got the feeling that most members have decided carnosine is not worth it, and could interfere with uptake of taurine (which they appear to find more important). Because of this discussion I now have a Kg bag of beta-alanine powder in my cupboard which I am hesitant to take, in part because I don’t want to take anything which I wouldn’t consider taking “forever” (also I like to layer things in slowly, and I just added 1mg daily oral finasteride several weeks ago with zero side effects thus far, including “interest/excitement” level). Also, since it doesn’t impact TMAO at all, if TMAO is found to benefit arterial AGE risks the use of carnosine shouldn’t negate potential benefits.
What is your opinion of carnosine to address your TMAO-related AGE concerns? And would it rank highly enough to make your “stack”?
As I see much of these lifespan/healthspan actions as trade-offs, I am focused on CVD as one area I would like to “overcompensate” for, given I am already addressing cancer risks with low-carb and metabolic health, and that the things that benefit with addressing cancer and CVD risk appear to improve blood flow and reduce kidney risks (so another major all-cause mortality risk being addressed) — now if I can just pay more attention when crossing the street. I have been considering a quarterly or half-year “pulsed” month course of Nattokinase as a protective factor for CVD plaque risks.
On the carnosine note, as I have a newly-diagnosed type-1 diabetic daughter, are there any thoughts on carnosine being appropriate for a 16-year-old to reduce the potential for AGE-related damage from serum glucose swings (inevitable for most T1D patients)? — her doctors have no opinion on this.
1 Like
@Ericross2 These are good questions that I am not able to answer. I am lining up a podcast with Dr Jed Fahey to get into the AGE details. I’ll know more about it then. As far as my personal efforts to date, I am focused on getting my blood glucose to low normal (from high normal). I am also working to reduce my protein intake (from high to normal), which will mean less salt water fish (related to TMAO). In addition, I eat a lot more vegetables & fruits (many benefits), eat fewer eggs, use more balsamic vinegar (helps with NO as well), eat little dairy fat, eat no added fat or sugar (only what is in whole foods), eat no red meat (except for a hamburger 1x / year), avoid frying and grilling…maybe that’s enough.
3 Likes
That sounds terrific, @Joseph_Lavelle . Your follow-up on this is much appreciated. If I can throw another possible question out for your podcast: is AGE-cross linked blood vessel based damage (lower elasticity) a separate issue from plaque-based arterial stiffness? Or are they related? — I’ve been trying to get my head around this, as well as how to stave these off (the inevitability). Same question for kidney disease/damage. Thank you.
3 Likes
@Ericross2 thanks for the suggestion. I’ll add it to the list. In the meantime, this study describes the many causes of arterial stiffness, including cross linking and calcification.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5308873/#:~:text=Arterial%20stiffening%20is%20a%20feature,cardiovascular%20risk%2C%20such%20as%20T2D.
2 Likes
A_User
#59
I don’t think that’s relevant or proves anything at all, if I am going to be blunt.
MR is miles ahead of such a study in proving causality.
LaraPo
#60
I eat only what I like and it happened to be a healthy diet. I dislike all kinds of meat, sweets, cakes, ice cream, and alcohol. I love good home made food and cook a lot.
When it comes to reducing the effects of AGEs, it would be interesting to hear pros and cons for pyridoxamine vs Beta-alanine.(not aiming at taurine’s interaction with beta- alanine)
Being blunt doesn’t make you right.
2 Likes
A nice talk that brings light on the question of low protein vs high protein.
3 Likes
A_User
#64
Well the study you cited is a mouse study. I cited a mendelian randomization study in humans which is like a natural RCT. They are two different leagues. The mouse study is near useless like all other mice studies, while the MR one is very powerful one able to assess causal relationships in humans. Likewise, mechanistic studies are very low on the evidence hierarchy, while MR is very high. This means the mouse study proves nothing and doesn’t give an alternative view, as it’s unable to do so by design. It’s just speculation for RCT’s or MR, which turned out false. It’s a hypothesis builder, not able to establish truths, and it was proven false by other ways.
Are totally with your process. I’m71 and have been on this path including annual nattokinase (neprinol 3x3 one month per year). I’ve been experimental on the diet and eschewing statins (“terrible” lipids, no plaques). I’ve been doing this for almost 16 years and have no physical issues. Fit and flexible. Workout with trainer 3x/week and do taiji the other 4 days (for 30 years). Married to 49 year old who can’t keep up with me 

2 Likes
Abstract
Age is a risk factor for numerous diseases. Although the development of modern medicine has greatly extended the human lifespan, the duration of relatively healthy old age, or “healthspan,” has not increased. Targeting the detrimental processes that can occur before the onset of age-related diseases can greatly improve health and lifespan. Healthspan is significantly affected by what, when, and how much one eats. Dietary restriction, including calorie restriction, fasting, or fasting-mimicking diets, to extend both lifespan and healthspan has recently attracted much attention. However, direct scientific evidence that consuming specific foods extends the lifespan and healthspan seems lacking. Here, we synthesized the results of recent studies on the lifespan and healthspan extension properties of foods and their phytochemicals in various organisms to confirm how far the scientific research on the effect of food on the lifespan has reached.
2 Likes
Dietary flavonoids intake contributes to delay biological aging process: analysis from NHANES dataset
Diet may influence biological aging and the discrepancy (∆age) between a subject’s biological age (BA) and chronological age (CA). We aimed to investigate the correlation of dietary flavonoids with the ∆age of organs (heart, kidney, liver) and the whole body.
4 Likes