A bunch of people tagged me. Tag back: @AustraliaLongevity @desertshores @cl-user
This is my very long-winded write-up, but I write to think, so it is what it is. I’m about 33% in sync with you, but I landed on a different overall approach that’s more cyclical and variable than the more common static approaches.
Of course, this is a very tricky subject with many variables, and there’s a lot of room for personal preferences and drug responses. So take this as a description of where I’ve landed for myself rather than as an attempt to prescribe an approach for anybody else. Still, it might inspire something for someone else, and the data are interesting to me.
It is long and detailed, though, so I’ll be amazed if anybody reads it to the end!
Data
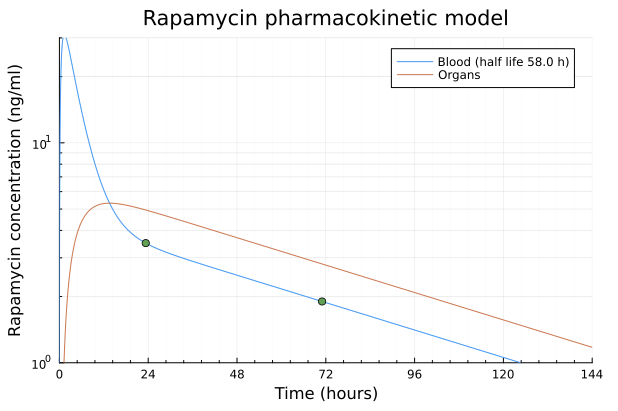
- My personal sirolimus half-life is ~54 hours for the exponential decay part of the curve. That is based on an 8mg dose with some nuts, no grapefruit. Eris/Biocon brand.
- Single 8 mg dose: 23.33 h = 3.5 ng/mL, 71 h = 1.9 ng/mL.
- Model that matches my labs: C(t) = 0.590 × dose(mg) × 2^(−t/54) (ng/mL).
- We will normalize some doses by my body surface area (BSA)
-
BSA normalized: 8 mg ≈ ~4 mg/m², 6 mg ≈ ~3 mg/m², 5 mg ≈ ~2.5 mg/m².
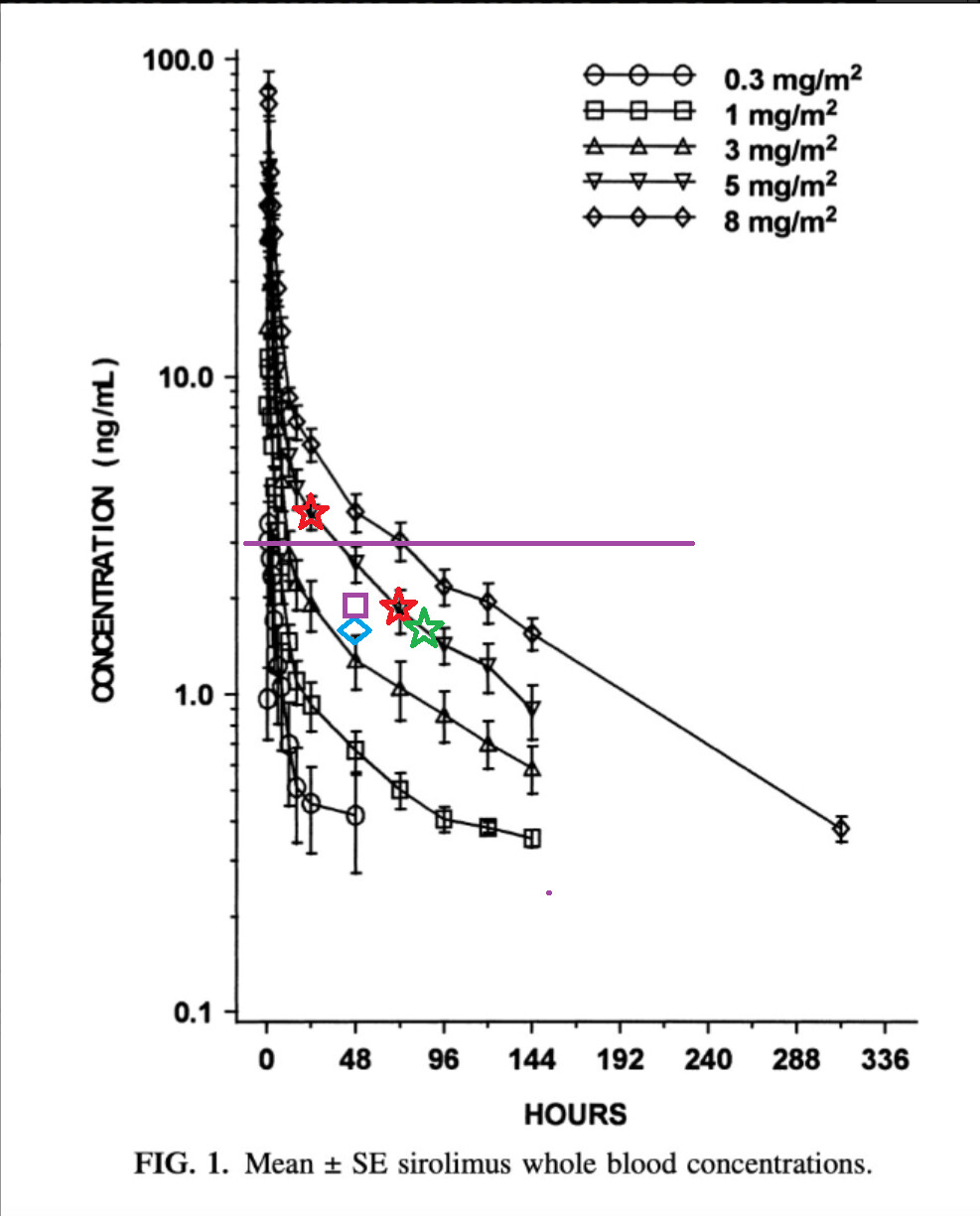
- Now, please reference the well-known blood concentration curve.
- The red stars are my lab results adjusted for BSA.
- The green star is a prediction at 84 hours (more on that later). 1.61 ng/mL
- The blue triangle is a 48-hour prediction based on a normalized 5mg dose. 1.59 ng/mL
- The purple square is a 48-hour prediction based on a normalized 6mg dose. 1.91 ng/mL
- Note how well my red stars follow the 5mg/m2 dose curve, though my BSA-adjusted dose was 4mg/m2. I will attribute this to different sirolimus formulations, my absorption of the drug, and variability in the BSA calculation, which is only an estimate.
- So why the green, blue, and purple calculated datapoints?
- Well, as stated elsewhere, I’ve run resistance training experiments at different doses and I’ve logged workouts for years. I have a decent sense of what is normal for me from week to week.
-
This is what happened during resistance training:
- At 5mg, 48 hours after the dose, my estimated blood concentration was at 1.59 ng/mL (blue diamond), and my training sessions seemed normal. Typically, that would involve some small progression of volume or load.
- At 6mg, 48 hours after the dose, my estimated blood concentration was 1.91 ng/mL (purple square), and I was clearly a little bit weaker the first session of the week, but I did better as the week went on. I still progressed week-to-week.
- At 8mg I was still weaker 84 hours after dosing, with an estimated blood concentration of 1.61 ng/mL.
- I went back and forth a little bit between doses to verify that the effect was real.
Conclusions about dosing
- How can we explain being fine at 5mg and 1.6 ng/mL but not fine with an 8mg dose at the same blood concentration 36 hours later? I am guessing that it’s the area under the curve and the time above the therapeutic dosing level, which we’ll assume is the purple line at 3 ng/mL.
-
Note that there is very little time above 3 ng/mL for the 5mg dose, assuming that the blood concentration scales linearly with dose. (It appears to on the plot and that would make sense to me if absorption isn’t dose dependent, but somebody smarter can correct me on that.)
- What I don’t know is what threshold I would have to drop below at an 8mg dose to be at full strength during training. I’m arbitrarily assuming something closer to 1 ng/mL.
- Note one more thing: To get above 3ng/mL for ~30% of the week, a goal discussed on this site, I would need a 10mg dose, which implies a very long RT interference period.
- Is this consistent with others have observed? I think so, because most here are taking relatively low doses. At the common 6mg/wk, recall that I experienced a relatively minor impact on my training, but I was still able to progress week-to-week. Clearly, there was some inhibition for me at 1.9ng/mL at T+48 hours, but it only slowed progress rather than halting it. So when others on the forum speak of being able to build muscle, or at least not regress, on similar doses, I believe it. I also think the progress being made is not what it could be if rapamycin were not in the picture.
What to do with this information
- What I wanted to do is determine how to apply these data to construct a training program that would also allow for regular rapamycin administration.
- The open question is when and how much to dose relative to training sessions that must meet some requirements.
- Of course, requirements vary with the objective. Do we want maintenance, slow-progress, or maximum hypertrophy or strength? Regardless, some of the constraints are the same, so let’s start there.
When to dose relative to the last resistance training session of the week
- The first thing I want to consider is when to take rapamycin relative to the last training session of the program cadence – let’s assume it is a program that aligns with weekly boundaries. Though 7 days is an arbitrary number, this kind of programming is the most common.
- What I want to consider is how long muscle protein synthesis can remain elevated after a good training session, assuming I am in a well-fed state with adequate protein. I am using a couple data points to derive some boundaries.
- In resistance-trained men (not beginners), muscle protein synthesis can remain meaningfully elevated for at least 29 hours post-training, in a protein-fed state:
- And resistance-trained individuals (even those with only a few weeks of training) will see their myofibrillar fractional synthetic rate drop to a level that is statistically equivalent to baseline (no training performed), after 48 hours, but still appears a little bit elevated. See figure 5:
- I am not interested in studies about beginners where MPS seems to remain elevated for longer.
- Ideally, I would want to avoid taking rapamycin inside a 48 hour window, or perhaps even longer, but I definitely want to avoid a 29 hour window, and probably a bit longer.
- For a maintenance or slow-progress objective, I conclude that waiting 36 hours after the end of the last resistance training session is acceptable.
- However, for a maximum hypertrophy goal, I would lean towards waiting a full 72 hours before taking rapamycin.
When to dose relative to the first resistance training session of the week
- The next thing I want to determine is how long I need to wait after dosing to have my first resistance training session of the week. This is obviously dose-dependent, and this is where I run into even more trouble.
- Consider this notional scenario:
- Day 0, 10 a.m., just finished my last RT session of the week. Now I wait 36 hours before dosing – here I am compromising on muscle protein synthesis.
- T+36 hours, call this Day 1, at 10 p.m., I take rapamycin.
- Now I am at the point where I know I can take a 5-6mg dose and have little to no perceived interference 48 hours later… yet I really don’t want to workout at 10 p.m. I have a few options: drop the dose even more, tolerate more interference by moving the workout inside the 48 hour window, or shift the dosing time earlier in the day on Day 1. No matter what, there is a compromise to be made.
- Let’s say I want to be cautious and I drop the dose down to 4 mg but keep the timing the same: at best, I’m getting a few hours (maybe minutes?) above the 3ng/mL therapeutic level. It isn’t even worth taking rapamycin!
- That isn’t an option. I want at least some appreciable amount of time, so I’m really back at a 6mg dose. The half-life calculation suggests I’d have about 13 hours above the therapeutic serum level. I know the pharmacokinetics aren’t that simple, but that’s the best I can do.
-
The question of whether this is even worth it remains. I get a few hours above 3ng/mL, and at the 48 hour mark I’m at 1.9ng/mL and feeling the effects, so I believe it did something. But is it enough? I don’t know. If I think of it as a caloric-restriction-mimetic, a 13 hours fast isn’t a big deal. I’d like to have at least 24 hours above 3ng/mL. Yet that implies that I need to take something closer to 7mg+, and then AUC becomes a problem, so I would have to push my first training session to the right.
Training program challenges
- Why push it to the right? Well, I don’t want to waste time training if I’m not going to get a good response or if I’m too weak to elicit a good stimulus.
- Now pushing it to the right might be fine except that I start to run into training programming issues. I’d have to drop from my present Upper, Lower, rest, Upper, Lower, rest, rest cadence to perhaps something like total body 2 days a week. Regardless, progress might be impeded.
- An alternate might be to just forget about the arbitrary weekly boundaries, but again, muscle group training frequency would decrease over any rolling time window.
- I think what I would do for a slow-progress goal is keep my 4 days of training per week and accept that I’m not getting nearly as much as I could out of rapamycin by essentially baby dosing at 5-6mg. I don’t like this at all.
Now what if my goal is maximum hypertrophy?
- This is much easier to think through because for this goal I want to maximize mTOR: I’m eating in a caloric surplus, eating a lot of protein (lots of leucine!) at frequent intervals, and I am unwilling to sacrifice muscle protein synthesis.
- In other words, for maximum hypertrophy I am all in and there is no place for rapamycin. It is completely incompatible with this objective.
- At this point I wonder what I’m left with. I can’t use rapamycin when I’m in a hypertrophy phase, and the dose I can tolerate in a slow-progress phase is so low I’m not sure it’s worth it.
So what dose do I really want?
- Well, 8-10mg gets me into the therapeutic range for about a couple days, which is pretty good. However, I know that it would interfere with resistance training for several days. Would that ever be okay? I think so, if my goal were simply to maintain muscle, because I wouldn’t need to train as frequently (say even one full body workout once a week). However, I could actually train more than one day a week with a higher dose if I consider another variable, as follows.
- With large doses, I would want to let my blood concentration drop back down to a very low trough level, so I would lean towards allowing 5.5 half-lives to elapse before dosing again. For simplicity, this means a 2-week cadence. The majority of the first week (probably 5-6 days), I am just doing cardio. After that, I do whatever resistance training routine I want, and I try to hit it frequently. Over, say, 8 days, I can get several training sessions in.
Final Conclusions
For me, rapamycin makes the most sense during a maintenance phase, and it makes no sense during a hypertrophy phase. It makes a little sense, but only a little, during a slow-progression phase.
So what do I want to do? I think I want to cycle through these three phases. Hypertrophy phases should be the shortest because I don’t want to live in mTOR-land for too long. Rather, I want to spend most of my time in the compromise zone where nothing is perfect, but I’m hedging my bets, banking on getting some small benefit from rapamycin while still building a little bit of muscle. I also want to spend some time in AMPK-land where I just try to maintain what I built up in the other phases, perhaps drop any fat I accumulated in the hypertrophy phase, give my body a break, enjoy autophagy, become cardio-guy. Here, I change to a cadence of every other week with higher doses and some unusual resistance training programming that is very close to one week on, one week off. In this phase, I know I’m getting something out of the high-dose rapamycin, but I also want to keep this phase relatively short because I’m not fully convinced that it’s good or necessary to constantly hammer mTOR into oblivion. I recall Matt Kaeberlein’s discussions about this.
Once I reach a muscle mass objective, I can drop hypertrophy phases, or they become very infrequent. At this point, I monitor how I’m doing with DEXA scans and spend my time in the other two phases. I think a lot of people on the forum are actually in this general zone, satisfied with their level of musculature.
Essentially, what I have described looks a lot like bodybuilding phases but with rapamycin incorporated at variable doses and durations. This approach hedges bets and emphasizes different pathways. Given that we really don’t know how to optimize the use of rapamycin, I like the idea of mixing things up.