The first dose-ranging experiment ( Estriol Experiment: Human Male: N of 1) was a learning experience, and I feel more “steady” and confident now.
In this experiment, I’m taking 3 mg of E3 (estriol) every other weekend, which consists of 3 days of dosing at 3 mg each day, alternating with a weekend of rapamycin. This means I’m doing something for longevity every week! I have 1 mg E3 tablets and take 3 tablets spread throughout the day, based on a comment by Dr. Fraser.
I’ve received my pre-dosing blood work results, which are attached.
The total hormone situation is more complex than I can fully understand, and I’m navigating it as best I can. To shed light on this complexity, I’ll be adding additional blood tests. The new tests I plan to introduce at the mid-term point are:
• Estrogen, Total: This is very confusing, and I’ll dive into this in another post.
• Estrone: I’m trying to understand anomalies in the total estrogen number.
• Cortisol, Total: Suggested by AI for insight into a major pathway.
• DHEA-Sulfate, Immunoassay: Suggested by AI for insight into a major pathway.
• AMH (Anti-Müllerian Hormone): Suggested by AI for assessing testicular health.
• Prolactin: Suggested by AI for evaluating pituitary/thyroid interactions.
• Leptin: Suggested by AI for exploring appetite suppression mechanisms.
• Dihydrotestosterone (DHT): Suggested by AI for insight into male hormone processes.
One blood test I’m no longer pursuing is progesterone, as during the dose-ranging phase, it remained consistently low and stable (0.6, <0.5, 0.7 ng/mL).
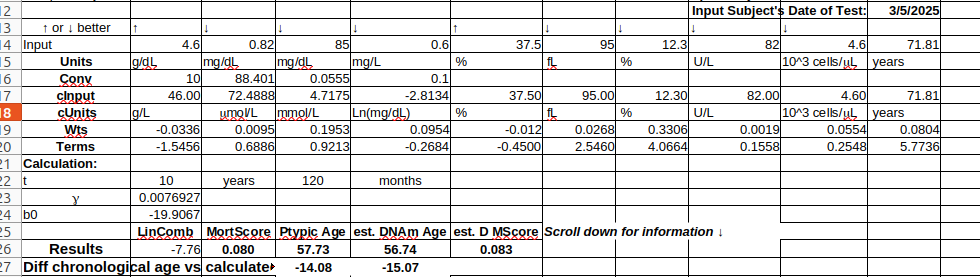
My Levine score is holding steady, showing a biological age approximately 15 years less than my chronological age.
March6_2025FullLipidHormoneREDACTED.pdf (238.8 KB)
4 Likes
Just looking at the measured sex hormones pre-dosing in both the dose-ranging and low-dose experiments, it appears they are numerically low but show significant increases across the board!
Leading up to the first dose-ranging experiment, I felt fine. My energy and libido levels were good. However, leading up to this low-dose experiment, I felt like I didn’t have quite as much energy, and my libido was okay but not great. Maybe I was just tired or not sleeping as well.
All of these blood markers increased, and I don’t know why. This was pre-dosing, with a 2-month gap between the end of the first experiment and the beginning of the second—about 4 months total.
• Estradiol: 17 increased to 28 (65%)
• FSH: 17 increased to 24 (41%)
• LH: 5 increased to 11 (120%)
• SHBG: 20 increased to 37 (85%)
• Free Testosterone: 36 increased to 57 (58.33%)
• Total Testosterone: 200 increased to 379 (89.5%)
I rounded the percentages and numerical increases, except for testosterone, because I know a lot of people focus on it. I have a friend who started TRT about 6 months ago, and he’s done really well on it. He’s lost weight, gained muscle mass, and has a happier, more positive outlook on life—you can even see it in the way he walks. If I showed him these numbers, he’d probably scoff. He’s an “800 T” kind of guy, and I’m happy for him, but I’m playing my own game.
1 Like
On my latest blood test, I somewhat accidentally ordered “Estrogens, Total, IA.” The reference range is ≤ 404 pg/mL, and my reading was 155 pg/mL. The lab shows this as within range, but it just doesn’t make sense to me. I was under the impression that this test measures E1 (estrone), E2 (estradiol), and E3 (estriol). My E3 levels never got above 0.20, and my E2 levels never exceeded 40. I don’t believe my E1 levels could be over 100 pg/mL.
According to some AI-provided data for females:
• Postmenopausal Females: ≤ 130 pg/mL (without hormone replacement therapy)
• Premenopausal Females:
◦ Follicular Phase: 60–250 pg/mL
◦ Ovulatory Peak: 150–750 pg/mL
◦ Luteal Phase: 60–400 pg/mL
Some references suggest a range for males of 10–50 pg/mL, which seems believable. For my next test, I’ve ordered E1 (estrone) separately to figure out what’s going on. It’s possible that E3 interferes with E1 in some strange way, but this is pre-dosing! This is now pre-dosing for the second experiment, and I find it very unlikely that E3 could have had such a significant influence several months after the last dose.
2 Likes
Summary Limerick:
A gent with his tests in a bind,
Found insurance less than kind,
The Combine said no,
To treatments, you know,
Now he switches his prickers each time.
I’ve started noticing some ripples from my recent lab testing. My insurance sent a letter noting I’d ordered blood tests typically used for transplant patients, asking for confirmation. I haven’t replied—seems I might be flagged in their system as a transplant case, which could complicate coverage down the line. (The bureaucratic gears grind on!) Meanwhile, my latest draw included both male and female markers, requiring me to sign two releases after confirming I understood the process, plus attracting several employees whispering and typing on the computer. So, these E3 experiments carry some risks—navigating the system being one of them. For my next round, I’m considering LabCorp over Quest. I’m not sure if it’s wiser to face one very irritated giant or two mildly peeved ones. Quest seems to be tightening the screws, so a switch might buy some breathing room.
2 Likes
Mid-Dosing Possible Side Effect: Muscle/Strength Stagnation
I’m about midway through this self-experiment with rapamycin and estriol, and I’ve definitely noticed at least some loss in my ability to gain strength and/or muscle.
My primary muscle exercise is training for the eponymous muscle-up—a pull-up over the bar followed by a dip on top. I’ve been working on it seriously for 3 years and casually for 5 years before that. I use an “assisted” weight counterbalance machine that provides a dialed-in amount of assistance. Currently, I’m at 13 lbs of assistance for a full range-of-motion rep. In a great month, with no interruptions like travel or family matters, I’ve gained up to 4 lbs of pulling strength, though 1 or 2 lbs is more typical. I’ve also been through tumultuous life periods where I’ve regressed.
Shortly before starting this experiment, I was at 14 lbs of assistance, where I could crank out 6 reps “easily”—probably 3 reps short of failure. At the end of those sessions, I’d often test my one-rep max if I felt pumped. On several days, I dialed it down to just 8 lbs of assistance, and one day I even managed 6 lbs.
Shortly after starting this experiment, I was at 13 lbs of assistance, but after several weeks, I’m struggling to get past 4 reps, which is noticeably slow improvement. Today, while resting between sets, I realized I’m slowing down on gains. Then it hit me: I haven’t “felt” like testing a max lift lately. The drive just isn’t there. I considered giving it a shot, but I could tell from how my muscles felt that any significant increase would lead to failure. Since it’s an over-the-bar move, failures need to be handled carefully—you could fall off and get injured—so prudence is warranted.
So, I’m definitely perceiving muscle “stagnation” on this dosing regimen. I’ve planned for a couple more weeks to finish up, but I need to think carefully about what this means for future tests. Decrease the dosing? Increase the spacing? I don’t know yet.
2 Likes
Got busted on an stupid AMH test. The first time I went into get tested for E3, I checked the neither male or female or both box or other box. I can’t remember exactly which one, but I knew if I checked male there would be red flags. This go around I got complacent, and checked male and when asked I told them I was male. Hey I could be gay, I could be a woman, prove me wrong.I could be a hermaphordite for all they know or can prove. Now I’m being sexually discriminated against. I think/hope the other hormone tests are going through. They always take the longest because they go to Puerto Rico.
TEST NAME: AMH
TEST CODE:
XXXXXXXXXX
CONTACT:
XXXXXXXXXXXXXX
Laboratory testing on this patient was verbally requested and/or confirmed by a physician or his or her authorized representative after contact with an employee of XXXXXXXX. Federal regulations require that we maintain on file written authorization for all testing. Therefor we are asking that the physician or his or her authorized representative sign a copy of this report and return it to the client service representative.
Signature:______________________
Note: The X’s represent identifying info and the wording has been altered but the meaning retained.
1 Like
Some of the hormones have come back; estridiol 22; estrone 23. So I hope my testosterone results are “approved” and make it through. I think I know what I did wrong. When the 2 extra people came in before the blood draw they asked “Who ordered this test?” I said I just bought it online. There is an actual ordering physcian on the paper. I should have memorized his name and said he is an old friend and personal physician. Lessons learned. Actually next time I start to feel “something is up” I’m walking out I’m not saying goodbye or by your leave or later dude or my phone rang and an emergency came up. I’m just walking out calmly, silently and quickly. Come to think of it, it’s time to ditch these guys and go with the competition.
Mid-Term Testosterone Results
Summary:
- Mid-term testosterone results show no change from baseline
- Muscle stagnation “light to moderate” rather than “severe”
- Similar experimentation ill advised in younger adults
The blood draw was on the Monday morning after the last weekend Sunday dose of 3mg E3. It’s basically a flat line from pre-dosing.
Free T 56.9=>57.4
Total T 379=>393
Also at the gym yesterday I did a 1 rep max with just 5.5lbs of assistance. And it was before getting my testosterone results so I wasn’t pumped because of the mildly good news. On the last set I leaned on the machine and told myself I can do this thing, up and over dude. So my report of muscle “stagnation” is somewhat moderated. My assessment is that I’m still in a “slow” time, but not really weirdly severe. I’ve been in “slow” times before. Classic limitation of N=1 experiments.
My leptin came back at 1.2 which is on the low side even for a thin old man. My pet theory is that the whole loss of appetite phenomena is central to the longevity mechanism exhibited by E3 and several other contenders. I might go ahead and do multiple pre/post leptin tests. Grok says it might take 7 runs to nail it down with proper methodology (same time of day, fasting, sleep,etc.)
Even with these encouraging results, E3 and rapa is “no country for young men” So I agree with Brian dropping Rapa. His young fans face a different calculus than I do, risking a lifelong loss in RHR or muscle AND immune risks—for a “possible” benefit of life extension some 50 years in the future. And adding a female hormone on top of that produces a risk profile totally unsuitable for young fathers starting a family. I’m a boomer, closer to the end, and I can clearly see the finish line. Young guys shouldn’t be the guinea pigs on this one—they’re already carrying enough with the economy tanking and wars and rumors of wars where they, not I, will be on the line. Let us old boomers scout out this wild and unknown country first. I feel honored to help shoulder this task.
1 Like
I think that younger people may benefit from taking rapamycin as part of an autophagy plan once a year, but weekly is a bad idea.
3 Likes
Yes, absolutely, I agree such a minimalist approach avoids the specter of constant bombardment. And young people are generally resilient. I’m not a doctor, but I think such a light touch would be very unlikely to cause any lasting harm. And of course under a doctor’s guidance some type of coordinated scientifically based, well monitored treatment plan might be great. But I ain’t there. I’m gliding solo on a wing and a prayer, scouting unknown territory.
1 Like
I consider 25 kind of the transition point to where a youth is fully mature, and for good or bad, fully capable of making their own decisions. There is the clearly dubious case of putting a healthy 18 year old on a lifetime of daily immuno-suppresants for possible future benefits. So there is a large grey area between the two. With my own offspring in their late 20’s I mentioned I was taking rapamycin for longevity and briefly suggested they might consider it, but that was it, and I never brought it up again. Recently one of my sons was in the kitchen when I was fussing about the complexities of E3 with my wife and he listened for a bit to get the jist of the conversation, then he just kind of shook his head and walked off.
Full Mid-Dosing Lab Report
The final lab report from my mid-term testing is in, and the last marker that straggled in last night—IGF-1, via LC/MS—might be the most intriguing thing I’ve stumbled across yet. It dropped from 152 to 120. Both are in range, but that percentage dip’s got my attention. The slight testosterone bump was odd, though IGF-1’s a bit off the sex hormone beaten path. A quick search hints lower IGF-1 might tie to longevity—significant maybe, but I’m in over my head here. Still, I’m pleased as punch, and IFG1 is locked into my blood work from now on as I try to figure this out.
Curious what the bio-experts here think—prime cause of appetite dropping off? Weird tweak keeping Leydig cells humming in the testes? Thyroid taking a nap? Thoughts?
P.S. Full disclosure: I ran this by GrokAI to my tone down my grumpy old man vibe:
Latest Mid Dosing
Pre-Dosing
Lastest Report
March31postdoseE3hormonesREDACTED.pdf (1.5 MB)
I think IGF-1 has legs, I’ll track it going forward.
From the linked article:
Taking all of this information into account, for most adults, keeping IGF-1 below 175 ng/ml is likely important, and below 150 ng/ml should be even more protective. Serum IGF-1 levels below 80 ng/ml may be detrimental, especially after the age of 75.
And I probably should have looked here first:)
3 Likes
For the pre-dosing, I used an old version of the Levine Calculator. I checked online at https://www.longevityworldcup.com/, and it gave me a reading of about -15 years. I then used the newer Levine version, which gave roughly the same result, so -15 years seems accurate for my baseline. I haven’t done the post-dosing test yet. If it doesn’t improve the numbers, I’ll need to rethink my course. The cute little mice in the ITP trials do tug at your heartstrings, so whenever they indicate something works, I do whatever I can to set sail with it. For example, I tried Meclizine for months at different doses, but even a few mg/day caused daytime weariness. I’m currently paused on acarbose because I’m working on my gut health and this E3 issue, but I haven’t abandoned it. I’ll revisit it at a lower dose or different timing once I navigate through these uncharted waters I find myself in.