I will give my standard reply: “If it ain’t broke, you can’t fix it!” So, everolimus would be the same in that regard.
Is there something specific you expected from sirolimus?
I have been taking it for 4+ years at higher-than-average weekly doses, and it has solved a multitude of old-age problems. (I am ~85 years old).
I agree that everolimus may be a better option for life extensions, but the jury is still out. I am not sure what benefits everolimus crossing the BBB would have, as my subjective view is that my brain is still fine.
I posed a rather lengthy query to paid versions of ChatGPT 5 and Gemini, basically asking to compare everolimus with sirolimus for life extension based on what is known. Dosage equivalents, blah blah blah.
The response was very lengthy, so I will just post a few relevant highlights. You can see the query and full responses in the links below. I prefer Gemini’s response.
Assessment: Is Everolimus a Superior Alternative for Life Extension?
- Strength of lifespan evidence
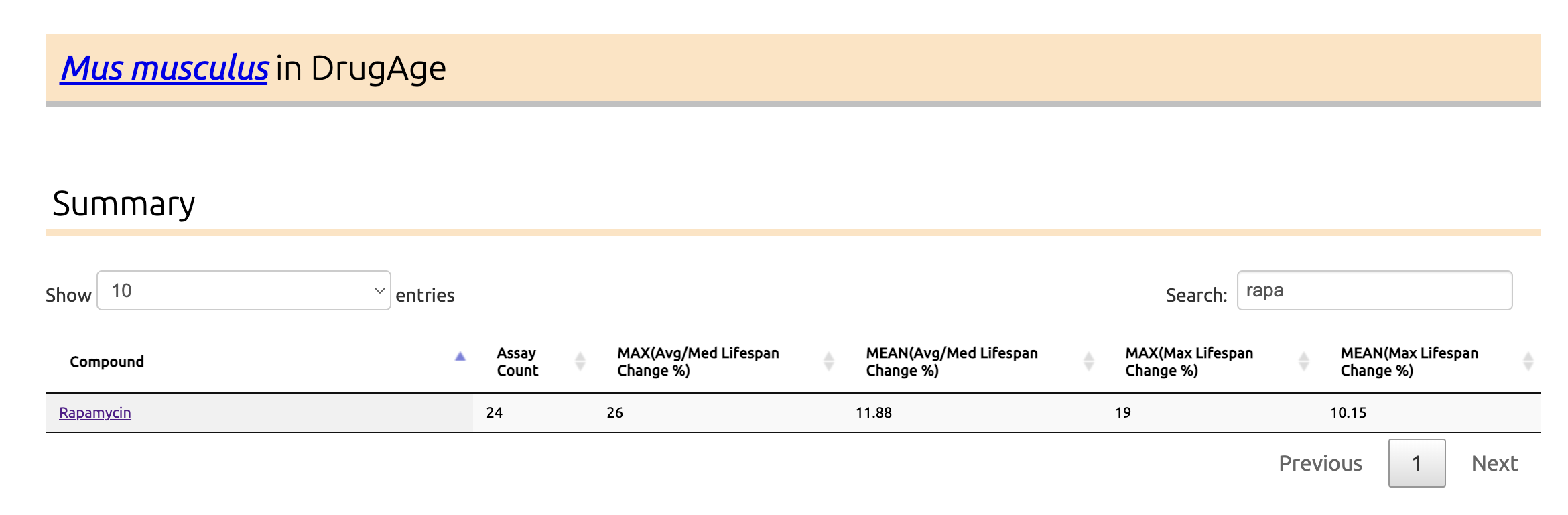
- Sirolimus (rapamycin) is, so far, the only drug consistently shown to extend lifespan in multiple mammalian studies (mice), across sexes, strains, and ages at treatment onset, with median lifespan increases often in the ~9–26% range and accompanying healthspan benefits. ScienceDirect+2OUP Academic+2
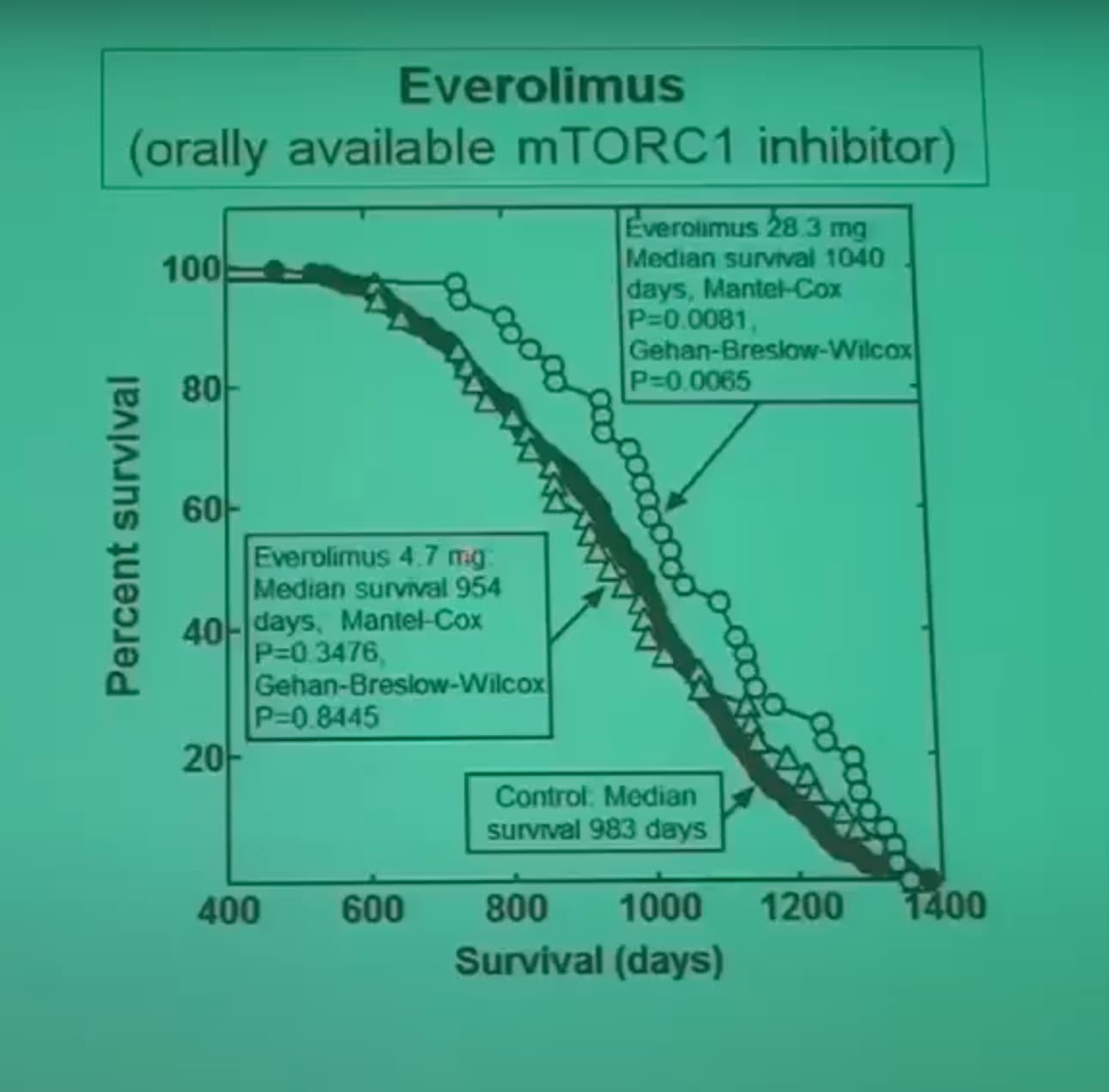
- Everolimus has robust anti-tumor and survival data in cancer-prone mice (e.g., Eμ-Myc lymphoma, APC^Min/+ models), but no published wild-type mouse lifespan program comparable to the rapamycin literature. Survival extension is usually framed as “delay of tumor progression” rather than “general lifespan extension.” AACR Journals+2ScienceDirect+2
- Current high-level reviews of mTOR inhibitors and aging repeatedly emphasize rapamycin as the agent with strong, reproducible mammalian longevity data, while positioning everolimus (and other rapalogs) as promising but under-tested in this specific context. lamminglab.medicine.wisc.edu+1
Everolimus (RAD001) has the best human immune-aging data: in older adults, low-dose regimens such as 0.5 mg/day or 5 mg once weekly for 6 weeks improved influenza vaccine responses (~20% better geometric mean titers) and reduced some infection endpoints, with acceptable short-term safety.
Similar “healthy-elderly immunosenescence” studies with sirolimus itself are fewer; most human sirolimus data come from transplant and rare disease populations, where doses and co-medications are very different from longevity practice.
However, transplant data broadly suggest that when adjusted to equivalent exposure, rapamycin and everolimus have very similar patterns of adverse effects (stomatitis, dyslipidemia, cytopenias, and infection risk), with modest differences between studies.
Some preclinical work suggests rapalogs (everolimus, temsirolimus) may produce less mTORC2-driven metabolic toxicity at certain schedules, but other data (and transplant experience) show broadly similar metabolic side-effect profiles when dosed to comparable efficacy. PubMed+2Nature+2
Blood–brain barrier and brain aging
- Both sirolimus and everolimus are lipophilic macrolides that do cross the blood–brain barrier, but CSF levels can be low and brain penetration is considered limited and heterogeneous. Nature+2Nature+2
- Everolimus is widely used in tuberous sclerosis and brain tumors, with evidence of central mTOR pathway inhibition, while rapamycin itself also has preclinical data showing CNS mTOR modulation. Cancer Care Ontario+2MDPI+2
- At the low weekly doses used for longevity (e.g., 5–8 mg sirolimus or ~5 mg everolimus), relative CNS exposure and functional impact are unknown, and no head-to-head cognitive-aging or neurodegeneration trials exist.
Overall judgment for someone on 6–8 mg once-weekly sirolimus
-
Evidence hierarchy:
- Sirolimus: strong mammalian lifespan data + substantial mechanistic and clinical experience.
Absorption and Bioavailability
Both drugs are substrates for the P-glycoprotein (P-gp) efflux pump and the Cytochrome P450 3A4 (CYP3A4) enzyme system in the intestinal enterocytes, which historically results in low and variable oral bioavailability.7 However, the structural modifications of Everolimus confer specific advantages.
Dosage Equivalence Scenarios
| Strategy |
Sirolimus Dose |
Everolimus Equivalent |
Rationale |
| Direct Weight Match |
1 mg |
1 mg |
Everolimus yields higher Peak, lower AUC. |
| Transplant (Trough) |
1 mg (Daily) |
1.5–2.0 mg (Daily) |
Compensates for rapid clearance to keep immunity low. |
| Longevity (Pulse) |
6 mg (Weekly) |
8–10 mg (Weekly) |
Ensures maximal autophagy trigger (Cmax) while utilizing rapid half-life for recovery. |
Is Everolimus a “Better” Option?
Affirmative, with qualifications regarding cost and evidence density. From a pharmacological perspective, Everolimus is the superior agent for “pulsed” dosing regimens. The primary criticism of weekly Sirolimus is its 62-hour half-life, which makes it a “dirty” pulse; significant drug remains in the system for the entire week, leading to potential chronic mTORC2 inhibition and metabolic derailment. Everolimus (28-hour half-life) allows for a kinetically “clean” pulse. It achieves a high Cmax to trigger autophagy and clears completely within 4–5 days, providing a physiological recovery window that Sirolimus cannot offer.
9.2 The Neuroprotective Verdict
For individuals prioritizing cognitive health, Everolimus is theoretically superior. Unlike Sirolimus, which may inhibit mitochondrial function in the brain, Everolimus has been shown to distribute into neuronal mitochondria and stimulate bioenergetics. Coupled with its ability to reduce neuroinflammation more effectively than Rapamycin in seizure models , it represents the more targeted choice for neuro-preservation.
My own take is that everolimus is probably superior for older people in that it seems to provide better anti-cancer protection and help for the aging brain.
Thanks to your post, I have been rethinking this and plan to give evrolimus a shot.
Both Zydus and Biocon of India produce everolimus, and it is available at reasonable prices from India, albeit more expensive than sirolimus.
As I said, the responses from both Gemini and ChatGPT 5 are several pages long.
You may read the complete reports from both. Here are the links:
Gemini: https://tinyurl.com/3w5ebkcb
ChatGPT5: https://tinyurl.com/37w36bd2