I started my TRIIM experiment in Sept of 2023;
Ipamorelin 400mcg + CJC 1295 noDAC 250mcg - 5 nights a week
DHEA - 75mg - 5 nights a week
Retatrutide - 2.0 mg weekly
A small improvement over 1 year in immune markers.
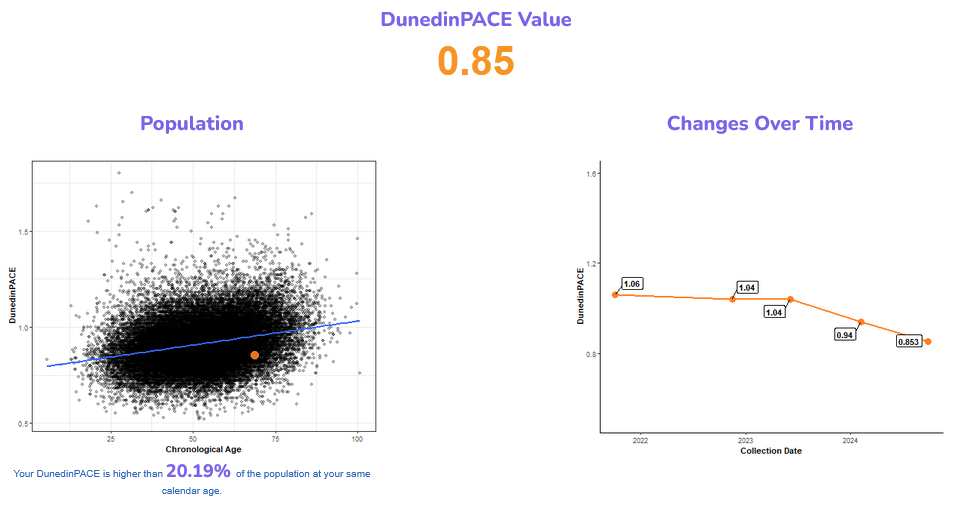
My last DunedinPace test was the best out of 5 so far. I’ll be getting another done in April.
5 Likes
Jjazz
#185
Isn’t HGH easily obtained from Indian pharmacies, just like rapamycin?
1 Like
LukeMV
#186
No because it requires an injection. Indian pharmacies don’t carry injectables.
Usually the places you can get HGH from also sell anabolic steroids, due to the fact bodybuilders take boatloads on HGH (much higher than the doses we are talking about here in TRIIM and TRIIM-X), hence the stigma around it.
3 Likes
Very cool, thanks @Steve_Combi! Off topic question about dosing : could you get similar benefits on a less frequent dosage? I’m thinking of something like 1mg ipamorelin and 2. 5mg CJC 1295, probably on different days. I know CJC 1295 has a longer half life, so it’s theoretically possible to dose it less.
My guess is that daily dosage is to mitigate blood glucose excursions from a bug dose, but there could be other reasons. Daily dosing also mimics very well what is done in the body, where GH is released every night.
2 Likes
With hGH secretagogues my objective is to enhance the circadian cycle of natural hGH production during sleep. Not concerned about glucose as the GLP1-R’s look after that.
Ipamorelin is typically maxed at 500mcg per dose. As I’m also interested in the other benefits of a more youthful level of hGH I’m not maxed on that one so I can maintain a more consistent level over time. That’s also why I use the noDAC version of CJC with the shorter half-life, so I can use it on a more regular basis. Because I can use both every night without concern about “accumulation” and potential loss of dose control, I mix them and only need 1 injection for this one 5 nights a week.
The pro-hormone DHEA seems to be an important part of the TRIIM protocol as well, it has a recommenced use range of 50 to 150mg so I picked the middle of the road 
3 Likes
LukeMV
#189
Even 50mg DHEA takes my DHEA-S level pretty high, especially when it peaks a few hours after taking it. The 24 hour trough level is on the higher end of the range so that’s about as high as I’d be willing to go.
3 Likes
Jjazz
#190
If the goal here is to mimic TRIIM, a growth hormone secretagogue should be titrated to a level that brings IGF1 up to at least 170 ng/ml. This is directly from Greg Fahy’s patent on the TRIIM protocol.
“For purposes of evaluating the suitability of a GH releaser for use in this invention, a fold change in IGF-1 level of at least 1.2 fold, or a final IGF-1 concentration of at least 170 ng/ml, are indicative of at least the potential for an adequate response.”
Life Extension offers an IGF1 lab for about $70. Test near the end of your 5-day cycle if you are using the typical 5 on / 2 off protocol. Personally, I’m happy to see an even higher IGF-1 level in the range of 250-300, closer to the upper end of the healthy range for a young male.
8 Likes
L_H
#191
You may well be right. However, its worth noting that immune function and t cell activity is maintained in adulthood long after thymus involution in adolescence. Suggesting that reversing involution should have long term benefits.
Also a “fully involuted” thymus has some function. This is suggested by the data on heart surgery patients - some had their thymus removed others didn’t and the consequences were dramatic for mortality.
We’re obviously guessing, but i would worry more about the long term consequences of high HGH than keeping my thymus in a adolescent state.
5 Likes
Ray1
#192
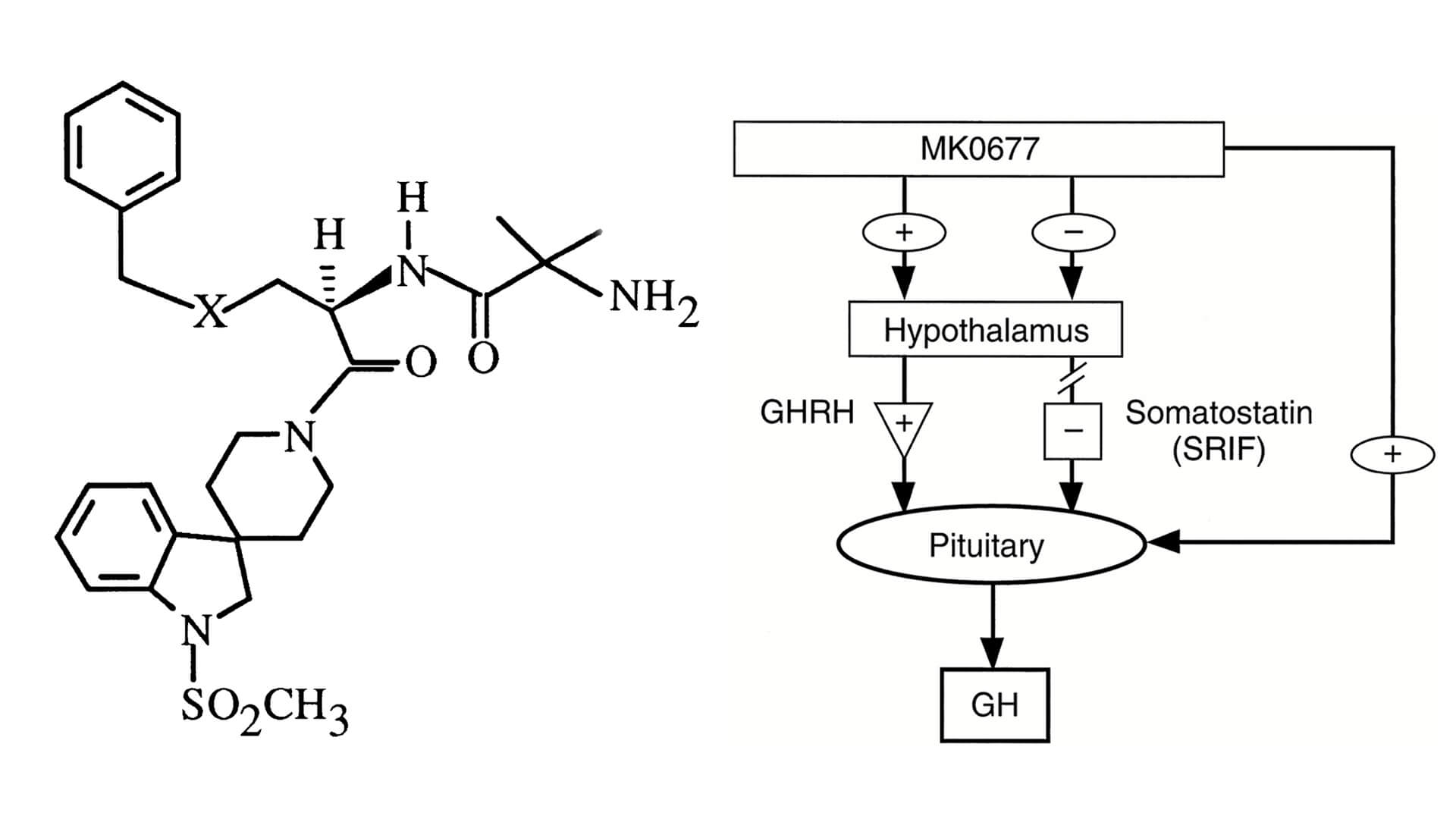
I just listened to the Attia podcast with Fahy. Toward the end, Fahy mentions that he might use a different drug in the he next version of the study to raise IGF1 instead of just using growth hormone. If he stated what drug he intends to use, I missed it. I wonder if it might be Ibutemoren MK677. Cheap and readily available.
5 Likes
Yes, T-cell activity is maintained, that is not the point of having a healthy Thymus
Maturation of new T-cells is the point. Once involution takes place the new T-cells, that are continuously being produced, do not go thorough the important maturation process that the Thymus provides. Three major thymus hormones, thymosin, thymopoietin, and thymulin become deficient in our 40’s… I’m well past that LoL!
As far as high hGH, I doubt that secretagogues are producing the same level of hGH as replacing the function with exogenous Somatotropin injections. Which is why I’m not concerned about that aspect. Making my pituitary gland do it’s job is different than replacing this function.
As with TRT, it’s been said many times in the past that TRT is not “healthy” as we age and yet today it is considered very healthy at rational levels. Instead of TRT, I do another secreteagogue Gonadorelin to make my boys get back to work
As we age “normal” ranges and levels of various hormones are “adjusted” due to statistics, mostly down It’s appears that may not be best way to deal with these changes, as in accepting this down regulation as “normal” seems to me to be counter intuitive in some cases, but not all.
6 Likes
L_H
#194
I’ll get reading, thank you
1 Like
L_H
#195
its top secret apparently. I imagine a patent application is pending
mccoy
#196
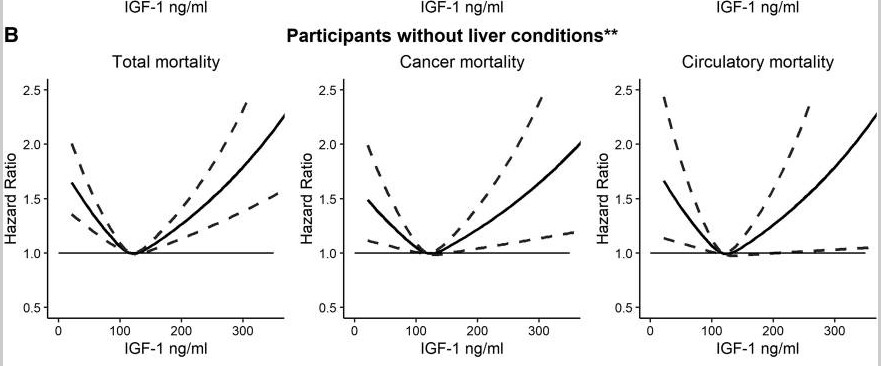
That sounds a bit of a gamble. The issue has been discussed in the podcast and Fahy is convinced that a higher IGF-1 does not imply higher cancer risk. However, a good part of the literature exhibits U-curve relationships where total, cancer and circulatory mortality HR are substantially higher above 200 ng/ml. Should we blindly trust Dr. Fahy and try to pursue the ideal target of 300 ng/ml, when this may, according to other sources, imply a 1.7 HR?
4 Likes
dicarlo2
#197
While I don’t entirely disagree with your point, the confidence interval at 300/1.7 is insane for circulatory mortality. And one can stop treatment should cancer show up.
1 Like
Neo
#198
Boosting growth factors, like IGF-1, for the rest of your life seems based on much/most of the mechanistic understanding of aging and longevity to be negative
If the goals is short term vitality, it might be good - but risks both decreasing long term helpspan and longevity
See also discussions about high IGF-1 etc elsewhere in the forum
Even the pioneer here, Dr Fahy, believe it should only be done on an infrequent basis and only for a vast minority of the total time.
5 Likes
mccoy
#199
Yes, and that’s a resounding YES, the plot on circulatory hazard can be discarded such is the scatter. Actually, should we be rigorous, only the total mortality plot has decent uncertainty far away from the optimum.
What all the graphs suggest to us in very eloquent terms though, is exactly what I said in the previous post: having a very high IGF-1 is a gamble. A potentially dangerous one.
Also, your point is true, close monitoring of cancer is necessary in these instances, but we all know that it is very tricky. Where is cancer going to manifest with max probability? Or should we implement a brute force strategy monitoring all organs, bones, tissues and so on? It can increase the cost and the commitment of the protocol significantly. And what if the above providing cancer masses are not so small that they cannot be detected. Liquid biopsy? Is it reliable since it’s such a newcomer?
Another point that adds to the complexity is that, as said above, Fahy’s protocol is intermittent, so the elevated IGF-1 state must not be kept chronically, but this takes us into unknown territory.
I’ll reiterate my question here: why no investor has shown up so far? Fahy’s protocol is well known and not a novel one. Maybe some investor has shown up, but not the important and reliable ones.
Bottom line: I still think that’s a fascinating hypothesis, but you would need a high risk appetite to undertake such a protocol.
5 Likes
Jjazz
#200
Great points and thanks for sharing the Mukama study. Full link below.
https://academic.oup.com/jcem/article/108/10/e1092/7124430
I should clarify - my reason for personally tolerating a higher IGF-1 level has to do with testing at the end of the 5-day cycle. Studies for some GH secretagogues have shown that IGF-1 levels will peak and trough with about 50-100 ng/ml of spread throughout cycles. So a peak at 250 may correspond to a trough at 150-200 ng/ml, ensuring that average levels are at or above the range Fahy suggests.
The positive associations for IGF1 and cancer are real and have shown up across many studies. So are the consequences of immune system collapse. Individual genetic and environmental cancer propensity should also factor into one’s risk benefit calculation when considering TRIIM.
3 Likes
Jonas
#201
Do Sauna twice a day to raise your IGF-1 instead.
LukeMV
#202
I haven’t personally used MK677 but have talked to many who have and some of them experience a little insulin resistance, water retention, and increased hunger on this. Not exactly things I’d want but I suppose it’s all about the dosage.
2 Likes
Rapan
#203
Exogenous hGH stops natural production of hGH. What’s the rate of successful reversal of growth hormone deficiency after 12-18 months of using exogenous hGH ?
I wouldn’t want to be dependant on exogenous hGH for the rest of my life.
Growth hormone secretagogues might be an alternative but not from a drug safety perpsective.
2 Likes