I asked my Dia AI browser to evaluate this information provided:
There is significant counter-evidence and debate in the scientific literature regarding the relationship between estradiol levels and cardiovascular disease (CVD) risk in men. Here are the main points of evidence that challenge or complicate the conclusions presented in the video:
1. Inconsistent and Heterogeneous Findings
- A 2024 systematic review found that the relationship between endogenous estradiol and cardiovascular endpoints in men is unclear and inconsistent. Out of 24 studies, 10 found no association between sex hormones and cardiovascular outcomes, 7 found associations for testosterone but not estradiol, and only 7 found a significant association for estradiol. The review concluded that the existing literature is heterogeneous and does not provide definite evidence for a pronounced net effect of estradiol on cardiovascular health in the general male population. The effect may be more relevant in specific subgroups, such as young and middle-aged white men, but is not generalizable.
2. Methodological Limitations and Confounding Factors
- Many studies are observational and cannot establish causation. Factors like age, obesity, and comorbidities are associated with both hormone levels and CVD risk, making it difficult to determine if estradiol itself is protective or simply a marker for other health factors.
- Measurement of estradiol is challenging due to assay variability, especially at low concentrations typical in men, which can affect study results and interpretations.
3. Potential Risks of Hormone Manipulation
- While some studies suggest that low-dose estrogen supplementation may improve vascular function in hypogonadal men, the long-term safety and cardiovascular effects of exogenous estradiol or testosterone therapy in men remain uncertain. Some trials have shown no improvement in atherosclerosis, and one reported increased coronary atheroma with testosterone therapy.
- Abuse of high doses of androgenic steroids (which can increase estradiol via aromatization) is associated with cardiovascular harm.
4. No Clear Clinical Guidelines
- There is no consensus or guideline recommending estradiol manipulation for cardiovascular risk reduction in men. Most clinical management focuses on traditional risk factors (blood pressure, cholesterol, diabetes, smoking) rather than hormone levels.
5. Need for More Research
- The evidence base is not strong enough to recommend for or against targeting estradiol levels in men for cardiovascular health. Large, randomized controlled trials are needed to clarify whether manipulating estradiol (or testosterone) has beneficial, neutral, or adverse effects on the cardiovascular system.
Summary:
While some studies support the idea that higher estradiol may be associated with lower CVD risk in men, the overall evidence is mixed, with many studies finding no association or being limited by methodological issues. There is no clear proof that raising estradiol improves cardiovascular outcomes in men, and manipulating hormone levels carries potential risks. Current best practice is to focus on established cardiovascular risk factors until more definitive evidence is available.
3 Likes
As Luke wrote and I agree on this… On one hand, I love that he (Kaeberlein) is bringing awareness to this.
I know the stigma, Matt kind of worried about it… and why he decided to put himself out there.
A few years ago I got a good bit of blow back for being on TRT… to achieve high normal testosterone levels. Several members PM:ed me for saying what they wanted to. But didn’t want the negative dialog.
Now, it’s just a normal course to improve health span as we age. Somebody has to be willing to correct the story… when it’s not only wrong… but actually hurtful to others who might benefit.
Matt will next be singing the praises of HGH. 
8 Likes
LukeMV
#23
It’s good that more and more people are becoming less ignorant to their mistaken belief that TRT is the same as a high dose testosterone steroid cycle. Those people still exists but we have made significant progress.
4 Likes
Since the topic is pretty narrow on this, only a certain segment might read these comments.
Curious how many on here (guys and gals) who are 40 and up thinking maybe I need this too … interested,or on the fence for hormone replacement.
And, what is keeping you from making the leap? Stigma, doctor approval, cost?
1 Like
I am being 100% honest. The reason: I cannot for the life of me find a reason to do so. And I have tried super hard. Muscles: I am an exercise hyperresponder - my muscles grow like crazy with any exercise, this was noticed even by my gym teacher at 14yo. He wanted me to go into sports, he said I was the best muscle responder he’d ever seen (but sports bored me). When I was preparing to work in Eastern Europe on a project with a bunch of friends, we wanted to get in shape first, so we hit the gym - it was insane how quickly I gained muscle, way, way faster than anyone else, got nicknamed mini-schwartzenegger. And so on, right till today - I gained muscle in my lower leg from isometric stands(!) alone. So testosterone for muscle - no need, thanks!
Mood. I feel fantastic. None of the usual complaints associated with low test. Not depressed, not anxious. No issues with motivation. Aggression level: pretty darn high in competitive situations (chess etc.). So test for mood - no need, thanks!
Bone health - not needed. Prostate - every PSA test except one at 1 or below, no issues with enlarged prostate and urination. Testosterone for any of this - no need, thanks!
I can find no data to the effect that TRT prolongs life or healthspan a la rapamycin - so since there are no measurable or implied benefits under the surface… why should I take it?
Literally, cannot find a reason. I’m 67yo and total test 444 ng/dL. Maybe higher would be better - but how would I know that? Again, to be very clear - I am not opposed to TRT in principle, and certainly don’t think others shouldn’t take it, or it causes cancer, heart disease, faster aging or whatnot, I have a positive opinion about TRT. It’s just that I cannot think of a reason for me to take it, and that’s reason enough for me not to take it. YMMV.
5 Likes
Wow… you  are an outlier no doubt.
are an outlier no doubt.
And you call me a mutant. Hahaha.
Although I might be a rapamycin super responder or perhaps started early enough and got good results before hitting the early 60’s aging acceleration.
I would concur. No need now… maybe swing back in a decade.
1 Like
Of course. If in the future TRT would benefit me - I’m on it immediately! Nothing stands still. Our bodies are constantly changing, and we have to keep adjusting. TRT might absolutely be in my future.
3 Likes
Most reasons I hear guys mention are:
- Hair loss
- Fertility
- Reliance on external source for hormones
- Dealing with doctors (this was a bother for me. Most doctors don’t take it seriously so it gets to a point where you can feel like giving up. This is where private clinics are good, or UGL if you’re feeling daring.)
- Stigma. This seems to be fading however. It’s not “cheating”, you’re only competing with yourself.
1 Like
LukeMV
#29
It I were in your shoes, I’d probably make the same choice.
1 Like
Exactly, at your age, if you are doing things half right no need.
Hahaha, why I said 40 or over at that first age bump. Things change, probably have all your kids by then.
1 Like
RPS
#31
My testosterone had dropped but I tried the Tonghat Ali supplement route to see if that helped before going for TRT.
The supplement boosted my level by 40%, so all the while that continues to work I’ll probably stick with that, but no qualms about moving onto TRT if the supplementation becomes ineffective.
2 Likes
What were your levels before and after? 40% is an impressive amount. The most I’ve heard tongkat increase testosterone was 100-150.
1 Like
RPS
#33
I’m away at the moment so can’t look up the exact numbers but from memory I had slipped below 300 and it got back up to something over 400 (all quite low but where I feel fine), so in absolute numbers you are quite correct with it being in the 100-150 range.
2 Likes
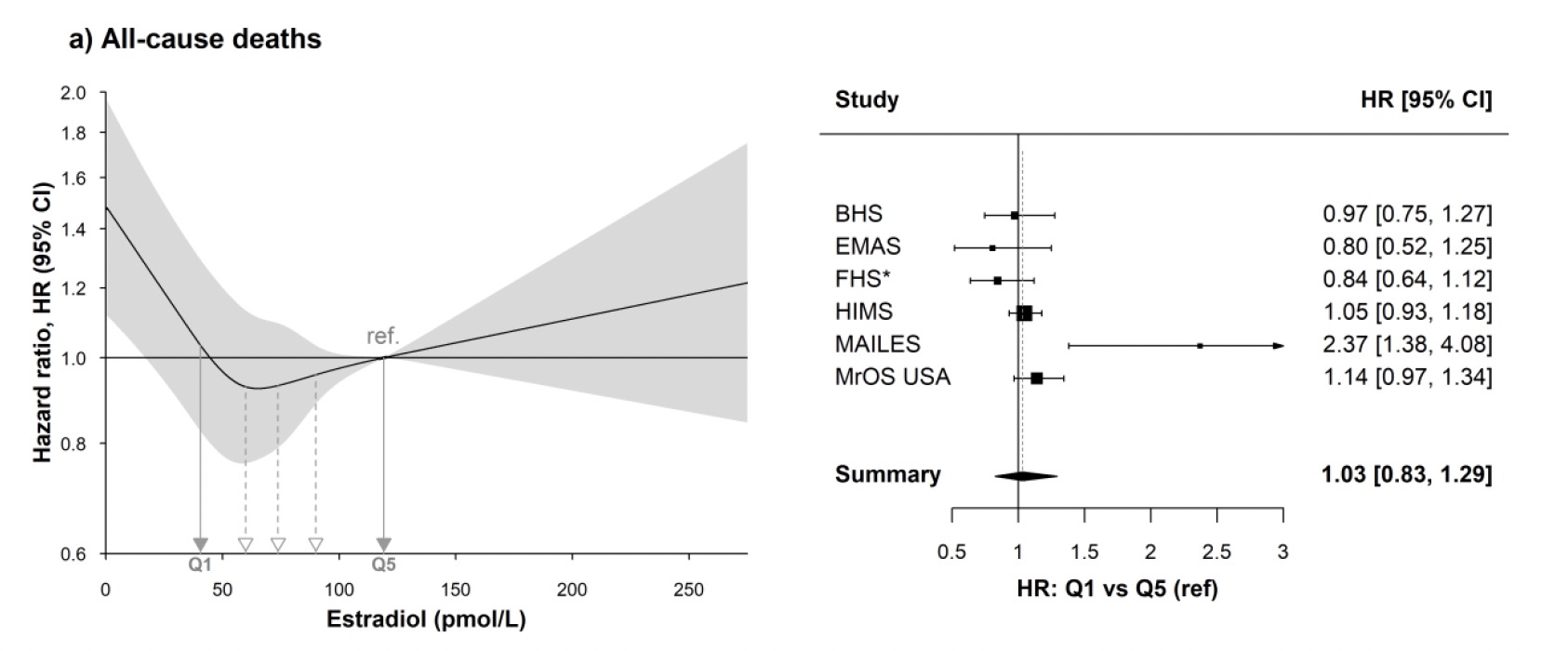
Putting aside the question of using anastrozole as such, Dr. Winge — who does put out some good content — is basing his conclusion on only a couple of studies here. A large individual-patient meta-analysis finds only very low levels associated with risk, with typical levels associated with low risk and high levels being either neutral or slightly harmful for total and CVD mortality.
(Don’t be fooled: the units here are in pmol/L, where standard US units are pg/mL. Q1 = 11.05 pg/mL, Q5 = 32.45.
He’s also inconsistent. First he says you can’t trust serum levels because local tissue levels can be disparate, but then he backs the claim that high estradiol is good for CVD based on serum levels.
2 Likes
Very low levels make you feel like you’re dying, so I’d avoid it just for that reason alone. The anecdotal body of evidence from the enhanced population suggests that “high” is best though of as relative to free T. The higher the free T, the higher people seem to like to have their E2. That has been my personal experience. My question about high levels in a non-enhanced or at least non-TRT-using population is whether the levels are high because of bodyfat, or is that a factor that was controlled for? In a normal-weight population with good insulin sensitivity and normal SHBG, how would E2 get too high? I wonder if this is a case of correlation rather than causation.
2 Likes
Thorin
#36
I am a man but from talking to my wife and other women, and from what I have learned, it seems to me that HRT is dramatically underused in women.
I am no expert at all but in my uninformed opinion, every woman should be on it once she hits menopause. Well, probably that is too strong, let us say every woman should have a conversation with a medical doctor with expertise in this area once she reaches a certain age.
Testosterone can definitely help many women. Obviously the dose taken is much lower than that taken by men.
6 Likes
Anecdotal evidence is always a contradiction in terms, but in what sense would you mean that it is anecdotally best? You don’t get anecdotal evidence for all-cause mortality. Or do you just mean that a lot of men (in general or on TRT?) feel better at higher E2?
That’s an intelligent question. As you can see in the abstract, “Covariates included age, body mass index, marital status, alcohol consumption, smoking, physical activity, hypertension, diabetes, creatinine concentration, ratio of total to high-density lipoprotein cholesterol, and lipid medication use.” (Before someone says “But LeBron James!”: aside from the fact that they adjusted for exercise, a recent NHANES study of 2,225 adults aged 20 to 59 confirmed that 97% of people adjudicated obese by BMI were obese on DEXA %body fat.
I would probably rephrase that to say that anecdotal evidence is a weaker form of evidence when compared to controlled or even epidemiological studies, but it’s hardly a contradiction in terms. Otherwise case studies would not be published in medical journals and we would stop talking about our personal experiences. There are and have been millions of men, and quite a few women, on supraphysiological doses of testosterone for decades, and we can learn a lot from their experiences given that studies at those doses are few and far between. That population truly provides the data available for certain compounds and doses, so I think we should make use of it, as limited as it may be.
That said, the consensus is that with higher levels of free T, supraphysiological levels of E2 are often better tolerated and provide a better subjective experience… up to a point. Gynecomastia tends to become an issue for many when estradiol approaches 60 pg/mL and acne before that. I don’t know how we could comment upon whether higher levels of E2 are protective in an enhanced population, though I suspect that given the frequent bloodwork obtained by many AAS users and the higher frequency of cardiovascular events, I bet some analysis could be done if only the data could be collected.
What is interesting to me is that unwanted side effects of both low and high estradiol are roughly correlated with the U-shaped curve for all-cause mortality.
OpenEvidence provides this summary that’s generally consistent with your reference. (Their references are at that link):
Higher endogenous estradiol levels in men, when controlled for confounders such as obesity, are generally associated with lower cardiovascular risk or a neutral effect, particularly in older men, though findings are sometimes inconsistent and may be influenced by age and BMI. Several large prospective cohort studies and meta-analyses support this, with some showing an inverse association between estradiol and incident cardiovascular events, heart failure, and cardiovascular mortality, especially in older or non-Hispanic White men. However, some studies report a U-shaped or nonlinear association, where both low and high estradiol levels are linked to increased cardiovascular and all-cause mortality, suggesting that mid-range levels may be most protective.[1][4-5][7]
Mendelian randomization and cohort data further indicate that higher estradiol may be inversely associated with risk of thromboembolism, ischemic stroke, heart failure, and silent myocardial ischemia, particularly in certain populations.[4-5][8-9] Conversely, a few studies have found higher estradiol associated with progression of subclinical atherosclerosis or prevalent coronary artery disease, but causality and confounding remain unclear; overall, the evidence does not support a pronounced harmful effect of higher estradiol in men.[2][6][10-11]
Most studies adjust for obesity and other confounders, but gaps remain regarding causality, optimal estradiol range, and potential ethnic differences. In summary, estradiol appears to be cardioprotective or neutral in men, with the possibility that both very low and very high levels may be detrimental.[1-11]
1 Like
blsm
#39
Thanks for your input Thorin. I’ve been on an estradiol patch for 8 years prescribed by my GP. I’m ready to get a more comprehensive hormone evaluation because there a few issues that estrogen alone hasn’t helped. I’ve tried a pea size amount of my husband’s androgel before and liked it (besides the one time I applied a little too much! Hahaha) I have a female neighbor and a relative that have an implanted testosterone pellet and that seems like it would be a good way go.
2 Likes
Thorin
#40
I can’t read the link due to not having the right permissions. I am wondering what % body fat by DEXA a man with a BMI of 32 needs to have in order to be adjudicated as obese?
I ask because that is my BMI. I am going to get another DEXA in a few months, but I’ve had it done 4 times over the years and I’ve ranged from 20% to 25%. I am anticipating a body at % towards the low side of that range in my next test.
1 Like