tananth
#41
Soft plaque on its own can cause blockage at the deposit site, which is responsible for 50% of heart attacks. While calcified deposits are older and probably stopped growing, they carry the risk of breaking lose in pieces and blocking small arteries elsewhere in the body and cause both strokes amd heart attacks.
1 Like
A_User
#42
What does ‘great’ mean?
It’s not probably what Peter Attia for example thinks is great… below 5th percentile, in the medical establishment. It is certainly atherogenic to have ‘normal’ levels, and all the evidence points to that.
Have you checked your Lp(a)?
1 Like
Jonas
#43
so what are the takeaways from your 4 years on rapamycin? biomarkers? energy level? visible signs? thanks!
I’m going to be doing a ton of testing in the next month, and adjusting my regimen - so will post a more exhaustive analysis when I’ve finished that, but briefly my experience of 4 years or so of rapamycin, and a couple years of acarbose / empagliflozin are follows:
Biomarkers: All trending positive except for lipids / ApoB (which I’ve always had issue with, even with a non-fat diet, but particularly bad on a Keto diet). So have restarted statins - and need to go in and get testing. Generally biomarkers good, Levine phenotypic age calculation down about 12 to 15 years below chronological age.
Energy Level: While on rapamycin - energy level great, like I felt when I was 30 years younger. I ended up taking about a 4 or 5 month break while doing a plasmapheresis trial (don’t know if I was on active or placebo arm of the trial) - and my energy really began to fall off after a few months. I suspect I was on the placebo arm of the trial.
Visible Signs: Hard to tell. Skin is great (I use rapamycin skin cream, and Retin A, and sometimes niacinimide and vitamin C serums on face.
More details after detailed testing this fall.
7 Likes
Jonas
#45
Thank you for sharing, looking forward to more updates. On the energy note, yes it happens to me too. Much more energetic with rapamycin than otherwise. Larry Ellison was quoted saying something similar about rapamycin and energy level in an interview a long time ago.
4 Likes
Thank you, @Joseph : this is an excellent summary paper. From it, the research cited suggests that people with existing plaques (probably all of us and we don’t yet know) can see substantial reduction in LDL and plaques (measured by the end products of fibrin/plaque degradation) at 6500 units of Nattokinase daily (for 26 weeks). For those of us without plaque, 2000 daily is fine. The Chinese study I cited earlier (not referenced in your overview) used 10,000 units daily for six months with strongly positive results.
One thing did bother me though: the paper breathlessly referenced a larger phase 2 clinical trial at USC which was expected to give more detailed results on atherosclerosis and dementia prevention in humans (at the time of publication it was still ongoing). However, when I searched for whether it had been completed, I found it was expected to finish in September 2019 but no paper has been published. Inconclusive results? — please publish or post whatever you have! (There’s a line that says “resuscitate submitted to clinicaltrials.gov in May 2023 so maybe they’re just reviewing the results. )
Nattokinase appears to reduce plaques, reduce LDL, reduce blood pressure, possibly stave off dementia/Alzheimer’s, and possibly more. I’ve been investigating this as a potential “solution” to my higher LDL numbers (my only health metric which is suboptimal).
While I eat low carb and a lot of meat/animal products (I’m just coming off a four-day fast this morning), I’m in the camp (ala Peter Attia) that believes lower/lowest LDL is probably best to reduce CVD and atherosclerosis risk; there’s some suggestion that higher LDL has some possible advantages if CVD/ASCVD risk is removed, so my thought is to reduce plaques with Nattokinase) and lower my LDL some via “natural” interventions (I’d prefer not taking a statin if I can, but only for “fear” of side effects which is somewhat irrational) but not PSK9-type reductions to the 5th percentile. Im already taking citrus bergamot (1000mg/day) and now cocoa daily in my coffee to try to bring my LDL down. Nattokinase addresses both the LDL and also plaque directly.
I’m finding it more difficult to resist adding Nattokinase to my stack, regardless of CAC scores.
4 Likes
What does ‘great’ mean?
It’s not probably what Peter Attia for example thinks is great… below 5th percentile, in the medical establishment. It is certainly atherogenic to have ‘normal’ levels, and all the evidence points to that.
Have you checked your Lp(a)?
“Great” pre-heart attack mostly meant “the doctor was happy” and did not recommend a statin, but the actual number for total cholesterol was generally 180 +/- 5 for ten years running and sometimes in the low 160s.
I never got Lp(a) checked before my heart attack. That’s one of those things where I didn’t know about it at all, and the doctor obviously never thought it was important enough to test.
3 Likes
A_User
#48
Your doctors never tested LDL cholesterol? Total cholesterol isn’t very accurate AFAIK.
1 Like
@RapAdmin Sorry if I asked this before but are you using a DIY made Rapa skin product or an off the shelf?
Yeah sorry they did test LDL, and that was usually 65-80. I was thinking about the NMR lipoprofile, which I’ve been getting done since the heart attack but didn’t even know about before.
2 Likes
I used my DIY rapamycin cream for 6 months, and now I’m using Healthspan’s rapamycin cream: Speak to a Doctor About Prescription Rapamycin (Sirolimus) Skin Cream
From a functional standpoint they both seem equal, but the Healthspan Rapa cream is a nice cream, feels good, and goes on well and I like the ECGC ingredient added. Full disclosure, Healthspan has given me a free subscription for it (for a few months) to try out.
4 Likes
A_User
#52
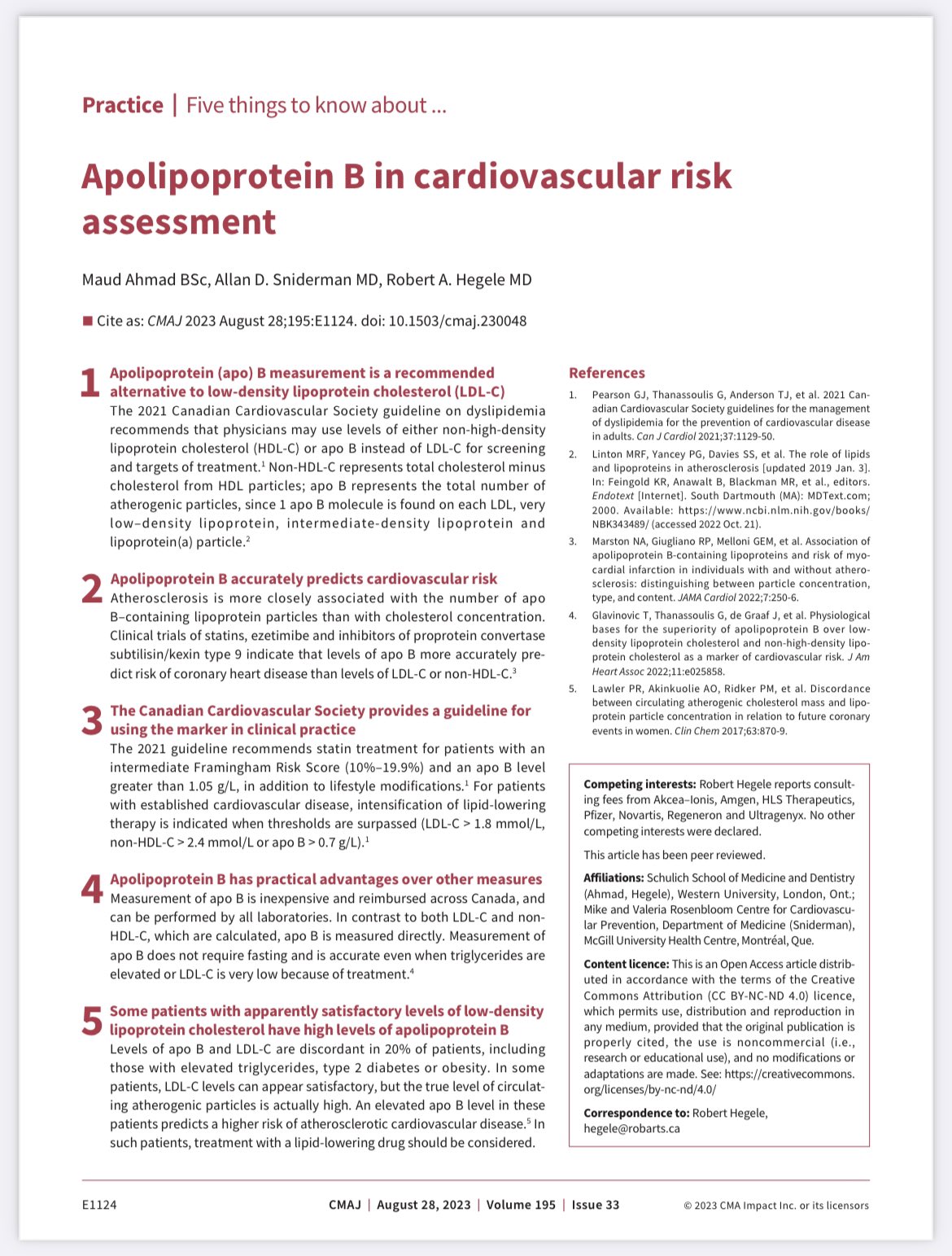
Your apoB or lp(a) could’ve been higher too. LDL isn’t really the cause only indirectly via apoB.
I don’t test LDL myself personally, only apoB and one time lp(a).
2 Likes
To be clear, a CT angiogram, at 10-20 times the cost of a CAC scan, is better in every way than the CAC- most critically it detects soft plaque. 15 % of those with an Agatston score of zero will still have soft plaque. As Peter Attia says, it is the better choice if insurance pays. It requires IV dye and slightly more radiation.
2 Likes
tananth
#54
The CT angiogram (including Cleerly) has 10x the radiation exposure of a CAC scan and should NOT be done annually just to monitor soft plaques. Use Cardiac MRI ($1000+ in USA, so around 2x the cost of a CT angiogram) instead which has zero radiation and the slightly better resolution for soft plaques than a CT angiogram.
A CT Angiogram (including Cleerly) is only recommended to assist with cardiac procedures (eg stenting), or if you cannot use MRI because of metal implants. In the latter case, you could consider CT Angiogram to monitor soft plaques, but not every year.
3 Likes
Mean effective radiation dose for a CAC scan nowadays is 1.05 mSv, and for CCTA, the median effective dose has come down to 2.88 mSv, so your numbers may need updating. Still, the CAC scan has 1/3 the radiation of a CCTA.
3 Likes
tananth
#56
In much of Europe (and possible elsewhere outside USA) the standard CCTA radiation dosage is 3x lower than in USA, so in Europe the CCTA radiation is about 3x that of CAC scoring as stated in your link , which state regarding CCTA radiation " The mean radiation dose from the newer generation CT used in 2019 was significantly lower than that of the single-source CT in 2010 (2.88 ± 0.85 mSv vs. 7.15 ± 3.4 mSv, p < 0.001)."
Why USA uses such high CCTA radiation levels (typically near the upper end of the older range 7.15 + 3.4 mSv) is unclear to me : possibly the CCT machines are not upgraded regularly like in Europe. I tried to find a center in USA that had one of the new low radiation Siemens CCT machines released in 2019, but could locate only a single one (in the Mayo Clinic), and Mayo Clinic probably only have one because Siemens donated it to them for testing (pre-release).
4 Likes
Is it going to change how I attack risk factors I can control? I’m still going to go all out
All tests like lpa and this can do IMO is make me paranoid and take away peace of mind
I’m still going to go all out on lipids/glucose/blood pressure etc as if my CAC was a known bad
4 Likes
Just checking San Francisco Bay Area options for this type of thing - will call and check some of them out over the coming months. I’m unsure of the value and may just work to get my ApoB down as low as possible:
CT Heart Calcium Score
This test checks for a buildup of plaque — made up of fat, calcium and other substances — which narrows your arteries and causes heart disease. This exam tells your doctor if you’re at risk for a heart attack before you have any symptoms, such as chest or back pain or tingling in your arms. Your doctor may recommend screening if you have a moderate risk of heart disease based on your risk factors.
Total cost: $156
Screening: $150 cash price Coronary Artery CT Scans available at leading California medical centers in 3 major metro areas (San Jose; Sacramento; and Los Angeles):
-
Stanford Health Care; LA BIOMED IN Los Angeles; and UC Davis Medical Center Preventive Cardiology are lowering the barrier to receiving the coronary artery calcium scan as a preventive screening test by offering it to patients for a cash price of $150 to receive this precision prevention information for understanding patients’ actual risk profile.
-
Stanford Health Care Radiology Wellness Screening Program
-
LA BIOMED Medical Center Appointment line: (310) 222-2773; HTTPS://LABIOMED.ORG/MATTHEW-J-BUDOFF-MD
-
Gundersen Health System:
-
UC Davis Health Referrals for CT Coronary Calcium:
- To Schedule appointments: Call 916-734-0655 or fax request to 916-734-2254. Include on fax or be prepared to provide on telephone: Full name, address, Date of Birth, telephone #, emergency contact (optional), Any Relevant Existing Diagnosis, Exam Requested: CT Coronary Calcium Scoring.
- Bring to test appointment: ID, Debit, Credit, or ATM card to be charged $150, or $150 cash.
https://rightcare.berkeley.edu/data-and-briefs/1379-2
Basic Vascular Health Screen
$460
- Cardiovascular health consultation
- Coronary calcium scan order and interpretation
- Carotid Intima-Media Thickness (CIMT) Ultrasound
- Optional 12-lead ECG
https://athleticheartsf.com/our-services/
3 Likes
tananth
#60
Excellent point : based on standard of care there is no benefit of getting a CAC scan unless it reveals an imminent over 70% clogged coronary artery, in which case a stenting procedure could save your life. However there are studies showing that aggressive LDL therapy without monitoring CAC score has better Total Mortality rates than aggressive LDL therapy + regular CAC scans : the reason is that too many patients showing partially clogged arteries are convinced by a cardiac surgeon to get a stent, long before it is really needed and every surgical procedure adds a low risk of death. Similarly every CAC scan, assuming a radiation dose of only around 1 mSv, adds a 1 in 20,000 chance of dying of cancer (in addition to a baseline average 20% chance of dying of cancer).
However, I learned in this group about OTC therapies like high dose Lumbrokinase that can dissolve plaque, but comes with a high likelihood of digestive discomfort and relatively high cost (around $6/day for 4 tablets/day of the most studied brand Boluoke). Possibly the optimal strategy is still to just take Lumbrokinase (+ Nattokinase and Serrapeptase with fewer side effects), without any CAC scan or CIMT ultrasound, if you can tolerate the digestive discomfort and the cost involved. In my case, I get mild diarrhea from Lumbrokinase, so I would need evidence of plaque from a CAC scan + CIMT ultrasound to motivate me to take Lumbrokinase for 6-12 months, though the 1 month/year followup treatment could probably be justified without any further testing.
4 Likes