L_H
#383
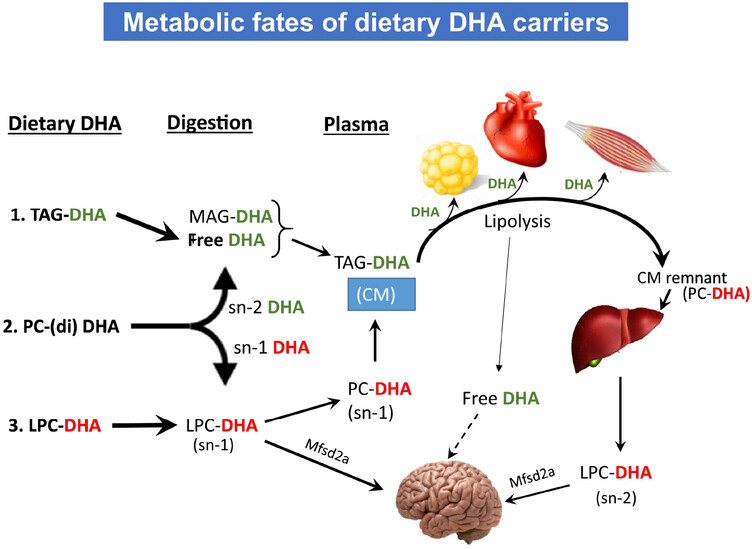
Thought this was interesting, in terms of target levels. The mouse study suggests quite a high dose of the best “lysophosphatidylcholine” form of DHA: 452mg. Or double that for the next best phospholipid form (phosphatidylserine) and 7 to 17x for the non-phospholipid form - triacylglycerol DHA (TAG).
If eating sardines that would require at least 2 tins a day?
“Using the allometric scaling [50], we calculate that the human equivalent daily dose of LPC-DHA for efficient brain enrichment is about 452 mg DHA for a 70 kg person, whereas the dosage using TAG-DHA, based on the previous studies, is about 3.4 g to 8.9 g of DHA per day.”
This metabolic pathway diagram is quite neat. But it suggests that the phospholipid-bound dha in Krill oil, containing being sn2 form won’t help DHA brain levels.
“Based on the results presented here, we conclude that the most commonly used carriers of DHA, namely TAG-DHA (as in fish oil), sn-2 DHA PC (as in krill oil) or ethyl esters (as in Lovaza®, Omacor®) do not enrich brain DHA, because they are absorbed as TAG, which is not efficiently converted to LPC-DHA in the liver”
1 Like
RobTuck
#384
My apology in advance if this was posted before. These short trials – 8 weeks in this case – irritate me but the findings are modestly positive.
2 Likes
A new paper (pointed to by @nicknorwitzMDPhD).
Lithium orotate, not galantamine hydrochloride, memantine, or rivastigmine, is the only medication that I know of that addresses prevention, symptoms, and possible reversal of dementia progression.
“https://www.youtube.com/watch?v=Hcz0Eyp1LE4”
Lithium deficiency and the onset of Alzheimer’s disease | Nature
4 Likes
L_H
#387
back on my hobby horse topic : “how much phospholipid-bound DHA is enough?”… this association (only) study I posted elsewhere suggests 4 portions of fish a week is better than 3 (the % relates to vascular brain disease in 75 year olds and is rather terrifyingly high!)
“Researchers found that among people who ate no fish, 31% had markers of severe underlying vascular brain disease, compared to 23% of those who ate three servings a week, and 18% of those who ate four or more servings of fish per week. This association between lower fish consumption and greater severity of markers of vascular brain disease was independent of any differences in brain volumes and other variables like age and sex.”
https://www.neurology.org/doi/10.1212/WNL.0000000000012916
3 Likes
Any updates?
Also:
Got my LDL results back, and they could be lower.
I did some reading on pterostilbene, and it can increase LDL, yet can possibly reduce Alzheimer’s.
Any info on this?
I’ll get round to it some time. Very busy time in the clinic + ER these days. Come the New Year will have a bit more time.
I think statins are a wonderful choice as it looks solid in regard to decreasing risk of AD, the longer you are on them the better. The recent Mendelian Randomization study saw >70% reduction, and with ezetimibe like mutations >80% reduction in AD. However, this would be the effect of using them lifelong.
Then over the short term, a well done trial looked like 60% rate reduction I believe (from memory) for ApoE4 carriers who went on a statin - albeit this was a short study.
I’d say skip the pterostilbene as if it has benefit, it’ll be small … treat the LDL / ApoB with a combination of Ezetimibe and a Statin would be my take on it.
As usual, consult your physician … but two drugs that hit your LDL, each of which decreases risk of AD … if worried about AD … I’d jump on that plan.
5 Likes
PREPRINT
Rapamycin enhances neurovascular, peripheral metabolic, and immune function in cognitively normal, middle-aged APOE4 Carriers: genotype-dependent effects compared to non-carriers
9 Likes
It would be nice for them to do a prospective trial with randomization into 1mg per day, 6mg per week, and placebo of each.
2 Likes
cfsrapa
#394
I saw a recent study on dual orexin receptor inhibitors clearing amyloid. Any thoughts on it being a potentially useful addition?
1 Like
Kidney Function, Alzheimer Disease Blood Biomarkers, and Dementia Risk in Community-Dwelling Older Adults
https://www.neurology.org/doi/10.1212/WNL.0000000000214446#sec-2
Quote:
“Impaired kidney function has been linked to altered concentrations of blood biomarkers of Alzheimer disease (AD), but the underlying mechanisms and its potential role in dementia development remain poorly understood. We explored the associations between estimated glomerular filtration rate (eGFR), blood-based biomarkers of AD, and dementia development.”
“The aims of this study were (1) to explore the cross-sectional association between estimated glomerular filtration rate (eGFR) and a comprehensive panel of AD blood biomarkers; (2) to quantify the hazard of dementia across different eGFR values over a 16-year period; and (3) to investigate the potential modifying effect of kidney function in the association between AD blood biomarkers and dementia.”
“The possible mechanisms by which kidney dysfunction alters the circulating levels of AD blood biomarkers are not yet fully understood—and include peripheral mechanisms, direct effects on neuropathology, or both. Indeed, it is plausible to hypothesize that reduced GFR impairs the peripheral clearance of these molecules, subsequently leading to an increase in their blood levels.35 Nonetheless, it is also plausible that a decline in kidney function is directly implicated in neuropathology,16,18 and that biomarker levels increase as a mere consequence of it. In fact, both the accumulation of uremic toxins and the release of neuroinflammatory cytokines that accompany CKD have been associated with neurotoxicity and nonspecific brain damage,17,36,37 which could contribute to dementia development. Of note, the older age and the higher comorbidity burden among participants with impaired kidney function might indicate the presence of underlying mixed brain pathology, which could also partially account for the elevated levels of biomarkers—especially NfL—observed in this subgroup.”
3 Likes
These agents are looking excellent to me. The issue is they are a controlled substance in the U.S., which requires a physician willing to Rx a controlled substance for prevention of AD … (which I will and am doing, but good luck getting this to make sense to your local Internist or Family Physician). Importation can result in criminal prosecution as it is a DEA scheduled agent. Albeit I really don’t see this as a addictive agent and think it has been misclassified.
Now on @CronosTempi 's post on kidney function this is complex and likely a couple of combined factors. To get significant decrease in kidney function, some unhealthy things have to be occurring in your body (including just getting older) and yes, many toxins and other inflammatory particles are renally cleared - knock down renal function - and yes, more of them remain. I would suggest that if one controls for these items, the kidney function decline is associated, but not the root cause of increasing AD risk.
4 Likes
59vw
#397
Would be great if you could post a link to the study.
My plan for individuals with ApoE4’s in regard to lab monitoring for progression (and this will evolve as additional tests come forward) is periodic (likely yearly for those not too adverse to the cost) of Beta Amyloid 42:40 ratio and p-Tau 217. This paired with the detailed brain MRI every 3 years with Neuroquant and yearly CNS Vital Signs, is what my approach is right now for monitoring. There are a lot of new tests coming forward, but most aren’t accessible and these ones have good evidence.
On the prevention side, I’m goaling for doing less things, especially on the supplement side. As much as one can make a decent argument for 100+ items on their own, the issue is the practicality and added benefit to adding item 101 to one’s growing list of drugs and supplements.
So my focused stack is:
Rapamycin cyclically with blood monitoring
SGLT2-i
Low dose GLP if tolerated
Telmisartan if needed
+/- items like Methylene Blue/NAD agents/NAC Ethyl ester
Statin
Ezetimibe
Low dose doxycycline and lithium
Dasatinib + Quercetin/Fisetin q2-3 months
Omega 3 optimization with agents that get into the brain
Homocysteine/Vitamin D optimization
I suspect that list gets 90% of any benefit on prevention based upon what I know right now.
Each of these agents has rationale, risks/benefits, and will be working through somewhat different pathways.
Lifestyle and making your brain do things it isn’t currently good at are huge factors. For example with CNS Vital Signs, what I’ve been doing is testing individuals, then picking out 2-3 areas of low %tiles on sections of the test, and then having them work on activities that specifically strengthen these … and retest yearly. Then pick another few low performing areas and make the brain work on these for the next year.
The low dose doxycycline is an interesting one - I’m going to put out a video on this one in the next month. It seems to make a lot of sense - but in sub-antibiotic dosing.
15 Likes
Beth
#399
Thank you for sharing your updated strategy.
I’d be very interested to learn more about Dasatinib / quercetin / fisetin if you are willing to discuss them.
2 Likes
adssx
#400
4 Likes
While it says “drugs” only 1 was tested, semaglutide in 2 large groups of 4,000 over 2 years with early stage Alzheimer’s.
More questions remain to be answered
• Wrong dose?
• Wrong timing?
• Wrong population?
• Not enough drug reaching the brain?
• Maybe GLP-1s help prevent, not treat?
• Or maybe we need better molecules entirely?
1 Like
Steve,
I think the issue is that once disease is present it’s a much tougher situation, we already have all the processes going with breakdown of the BBB, irreversible damage, etc.
I’m not seeing anything that looks that great for reversal of disease. There are some things that might help slow progression - but I’m not sure much in the prevention bucket will do much.
In the Mendelian Randomization review of Statins and Ezetimibe … looks like AD were 70+% and 80+% decreased respectively. I don’t think either of those will do anything once there is established disease.
My assessment at this point is monitor for very early disease (e.g. Beta Amyloid 42:40 ratio, p-Tau 217) and if any abnormalities, get aggressive to do everything to prevent progression.
Just like with sirolimus, we have a lack of data, and lots of anecdotes. We have a lot of data associating GLP-1 use with less diagnoses of AD - but association isn’t causation, but it is the best we have right now. The GLP-1 manufacturers need to get a bunch of ApoE4 homozygotes and start them on GLP-1’s age 60 … and a group at age 50 … there would be some answers in 10 years, as the control for both would have progression with their labs, even if not symptomatic disease as, I believe about 90% of ApoE4 homozygotes will have abnl B-Amyloid and P-Tau by age 70.
7 Likes