Part 3: Actionable Intelligence
The Translational Protocol (Intervention: Nicotinamide Riboside - NR)
Selected due to GRAS status and superior safety data density.
1. Human Equivalent Dose (HED)
-
Rodent NOAEL: 300 mg/kg/day (Conservative NOAEL from toxicity studies).
-
Conversion Factor: Rodent Km (6) / Human Km (37) = 0.162.
-
Math: $300 mg/kg times 0.162 = 48.6 mg/kg HED.
-
Calculated Dose: For a 70 kg human: 48.6 times 70 = 3,402 mg/day
-
Analysis: The standard supplemental dose (300 mg - 1000 mg) is well within the safety margin, representing <30% of the theoretical safe limit.
2. Pharmacokinetics (PK/PD)
-
Bioavailability: 60-90% absorbed, but extensive first-pass metabolism in the liver converts much of it to Nicotinamide (NAM).
-
Half-life: Plasma levels of NR peak at ~3-4 hours; NAD+ levels peak at ~8-12 hours post-ingestion.
-
Target Engagement: Increases PBMC (blood cell) NAD+ by ~60% with chronic dosing (1000 mg/day).
3. Safety & Toxicity Check
-
NOAEL: 300 mg/kg (Rats).
-
Phase I Profile: Safe up to 2000 mg/day in humans for 12 weeks.
-
Liver/Kidney: No hepatotoxicity observed (unlike sustained-release Niacin). No significant CYP450 interactions reported.
-
Warnings: Caution with active malignancy (theoretical risk of fueling tumor metabolism).
4. Biomarker Verification Panel
-
Efficacy Markers:
-
Tier 1: Whole Blood NAD+ (Direct measure).
-
Tier 2 (Downstream): Intracellular Acetyl-Carnitine (mitochondrial flux), IL-6 and hs-CRP (reduction suggests anti-inflammatory effect).
-
Safety Monitoring:
-
Homocysteine: High-dose B3 processing can deplete methyl groups. Monitor Homocysteine; if elevated, stack with TMG (Trimethylglycine).
-
Liver Panel: ALT/AST (Standard precaution).
5. Feasibility & ROI
-
Sourcing: Commercially available as Nicotinamide Riboside Chloride (Niagen). High stability.
-
Cost vs. Effect:
-
Cost: ~$45–$60/month for 300 mg/day; ~$120/month for 1000 mg/day (High Dose).
-
ROI: Medium. The “feeling” is subtle. ROI is highest for older (>50) individuals or those under metabolic stress.
6. Population Applicability
-
Contraindications: Active cancer (tumor turnover concern), Gout (theoretical, though less risk than Niacin), severe methylation defects.
-
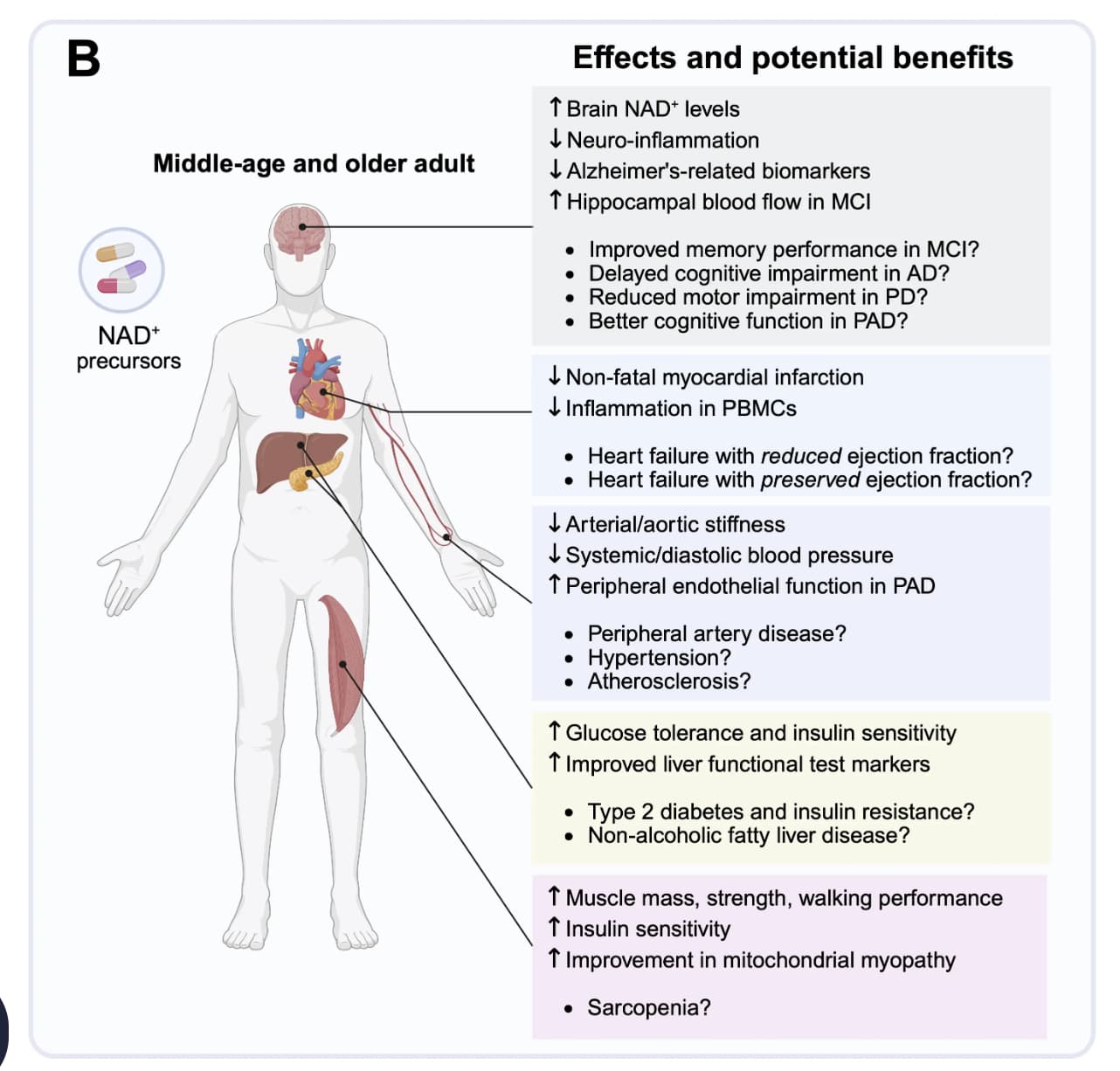
Best Candidates: Age 45+, History of metabolic stress, Heart Failure, Neurodegenerative risk.
Part 4: The Strategic FAQ
1. Does taking NR or NMN actually extend human lifespan?
Answer: Data Absent. There is no clinical evidence that NAD+ precursors extend human lifespan. We are extrapolating from mice (10-15% extension) and biomarker data (improved DNA repair/metabolism). It is a probability bet, not a guarantee.
2. Should I take NR or NMN? Which is better?
Answer: The scientific consensus is split. NR has better clinical safety data and GRAS status. NMN requires a specific transporter (Slc12a8) whose prevalence in humans is debated. NR may enter cells more easily by converting to NMN intracellularly. Currently, NR is the safer regulatory bet; NMN is the “high risk/high reward” biohacker favorite.
3. Does this conflict with Rapamycin?
Answer: No, it appears synergistic. Rapamycin inhibits mTOR (mimicking starvation), while NAD+ precursors activate Sirtuins (mimicking energy abundance/exercise). Both pathways converge to improve autophagy and mitochondrial health. Animal studies suggest the combination is safe and potent.
4. Does it conflict with Metformin?
Answer: No. Metformin activates AMPK; NAD+ activates Sirtuins. These are complementary longevity pathways. Some data suggests Metformin + NR reduces tissue aging markers more than either alone.
5. I heard NAD+ supplements deplete methylation. Is this true?
Answer: Plausible. The body eliminates excess Nicotinamide via methylation (creating Methyl-NAM). High doses could drain your methyl pool (betaine/SAMe), potentially raising homocysteine.
Fix: Take 500-1000 mg of TMG (Trimethylglycine) with your NAD+ booster to support methylation.
6. Will this fuel cancer growth?
Answer: Theoretical Risk. Cancers are metabolically active and love NAD+. While precursors don’t cause cancer, they might accelerate the growth of an existing tumor. Avoid if you have active cancer.
7. Why not just take Niacin (Vitamin B3)? It’s cheaper.
Answer: Niacin (Nicotinic Acid) causes a skin flush that some people don’t tolerate well, at the doses needed to boost NAD+ (500mg+). It also works via a different pathway (Preiss-Handler). NR/NMN bypass the flush and use the Salvage Pathway, which is more efficient for non-liver tissues.
8. Is the intravenous (IV) NAD+ drip better than pills?
Answer: Debatable. IV floods the plasma, but NAD+ is a large molecule that struggles to enter cells directly. It likely gets broken down into precursors (NR/NAM) in the blood anyway. Pills (NR/NMN) provide a steady trickle of precursors that cells can take up via transporters. IV is expensive and transient; oral is sustainable.
9. What is the optimal time of day to take it?
Answer: Morning. NAD+ levels follow a circadian rhythm (governed by the clock gene BMAL1). Levels naturally peak in the morning. Taking it upon waking mimics the natural cycle; taking it at night might disturb sleep architecture (energy boost).
Comparative Analysis: The Hierarchy of NAD+ Precursors
Topic: Niacin (NA) vs. Nicotinamide (NAM) vs. Nicotinamide Riboside (NR) vs. Nicotinamide Mononucleotide (NMN).Audience: Longevity Biohackers & Clinicians.
Part 1: The Executive Summary
For decades, Vitamin B3 (Niacin and Niacinamide) was viewed merely as a pellagra-preventative. Today, it is the ammunition in a biological war against aging. However, not all B3s are created equal. While standard Niacin (NA) and Niacinamide (NAM) can raise blood NAD+ levels, they face metabolic roadblocks that newer precursors (NR and NMN) are engineered to bypass.
The critical distinction lies in pathway efficiency and tissue specificity. Niacin (NA) is limited by the “flush” and its inability to fuel muscle tissue directly. Niacinamide (NAM) is cheap and abundant but relies on the enzyme NAMPT —the very enzyme that declines as we age, effectively creating a bottleneck in the salvage pathway. NR and NMN act as “backdoor keys,” entering the cycle downstream of these bottlenecks to forcefully restore cellular energy in aging tissues. In the hierarchy of longevity, standard B3s are “maintenance” for the young, while NR and NMN are “restoration” for the aging
| Feature |
Niacin (NA) |
Niacinamide (NAM) |
NR / NMN |
| NAD+ Boost Efficacy |
Moderate (Liver focus). |
Moderate (Systemic). |
High (Multi-tissue). |
| Pathway Dependency |
NAPRT (Absent in muscle). |
NAMPT (Declines with age). |
NRK / NMNAT(Resilient). |
| Sirtuin Activation |
Neutral. |
Inhibitory (at high serum doses). |
Activatory (via NAD+ boost). |
| Key Side Effect |
Severe Flushing(Prostaglandin release). |
None (Hepatotoxic at extremely high doses >3g). |
None known. |
| Lipid Benefits |
Excellent (Lowers LDL, raises HDL). |
None. |
Mild/None. |
| Cost |
Extremely Low ($). |
Extremely Low ($). |
High ($$$). |