There are twice as many people in the treatment group as on placebo. Check out the number right next to it.
3 Likes
Right: Look at the top of the columns. There are 110 people on placebo and 236 people on Obi. The numbers for each outcome are first the absolute number (n) and then the percentage (%) of the subjects in that group who had the event. Obi is nominally lower for everything, though there aren’t statistics in this screenshot.
2 Likes
Bicep
#148
Thanks to all. I’ve had a really busy day and just got back to look at this. It’s a couple percent better at all those, should gain traction for small LDL, lp(a), aboB, and several others. Looks like a good drug. It looks like they mostly tested it on people already on statin. Very interesting to see what happens without.
1 Like
adssx
#149
Check this larger trial, after just one year there’s positive (but not statistically significant) signal for all-cause mortality: Obicetrapib (CETP inhibitor for dyslipidemia) - #131 by adssx
2 Likes
Has anyone tried to purchase Obicetrapib from Indian vendors?
It’s not available as a drug yet. It’s still in the experimental stage.
1 Like
NewAmsterdam Pharma Announces Positive Topline Alzheimer’s Disease Data from BROADWAY Clinical Trial
PDF Version
– Pre-specified analyses show that obicetrapib treatment leads to statistically significant and clinically meaningful reductions in the primary outcome measure of Alzheimer’s disease biomarker in both the full ITT population (p<0.002) and in ApoE4 carriers (p=0.0215), supporting the emerging link between CETP-inhibition and prevention of AD pathology –
– NewAmsterdam to present results during the AAIC conference in July –
… The pivotal Phase 3 BROADWAY study was primarily designed to evaluate the low-density lipoprotein cholesterol (“LDL-C”) lowering efficacy of obicetrapib in adult patients with established atherosclerotic cardiovascular disease (“ASCVD”) and/or heterozygous familial hypercholesterolemia (“HeFH”), whose LDL-C is not adequately controlled, despite being on maximally tolerated lipid-lowering therapy. As part of this pivotal registration trial for lowering LDL-C, a pre-specified sub-study was conducted to assess the effect of obicetrapib on plasma biomarkers of AD in both the full study population and in patients carrying the ApoE4 gene. …
A total of 2,530 patients were randomized 2:1 to receive 10 mg obicetrapib or placebo dosed as a once-daily oral treatment, with or without food for 52 weeks. The mean baseline LDL-C for enrolled patients in the obicetrapib arm was approximately 100 mg/dL despite high intensity statin use reported by nearly 70% of patients during screening. Females comprised approximately 34% of the trial population and the median age of participants at baseline was 65 years.
The primary endpoint was LS mean percent change from baseline in LDL-C of obicetrapib 10 mg compared to placebo after 84 days …
Alzheimer’s Sub-Study Trial
In BROADWAY, a pre-specified AD sub-study was designed to assess plasma AD biomarkers in patients enrolled in the BROADWAY trial and evaluated the effects of longer duration of therapy (12 months) with a prespecified population of ApoE3/4 or 4/4 carriers. The sub-study included 1727 patients, including 367 ApoE4 carriers. The primary outcome measure was p-tau217 absolute and percent change over 12 months. Additional outcome measures included neurofilament light chain (“NFL”), glial fibrillary acidic protein (“GFAP”), p-tau181, and Aβ42/40 ratio absolute and percent change over 12 months. NewAmsterdam observed statistically significant lower absolute changes in p-tau217 compared to placebo over 12 months in both the full ITT population (p<0.002) and in ApoE4 carriers (p=0.0215).
No quantitation of the effect size, or the relative effect in carriers vs. noncarriers (and the carriers were less powered than noncarriers), or the effect on neurodegeneration-adjacent markers.
6 Likes
Already extensively discussed -
3 Likes
José
#157
That was in February 2024
1 Like
It is not obvious how to read that graph.
1 Like
adssx
#160
I looked at that graph for a long time, but then I gave up, thinking that no one knows what these AD biomarkers are or whether having them up or down is better. I want to see the impact on cognition. The rest is noise.
4 Likes
It does seem like they messed up that diagram in the rush to get the news out. If it delayed progression of the marker and was more potent in the ApoE carriers, then why is the marker more positive while being lower or even negative in the placebo group?
Maybe it’s supposed to represent “% inhibition of progression”? This, more positive and higher is better.
1 Like
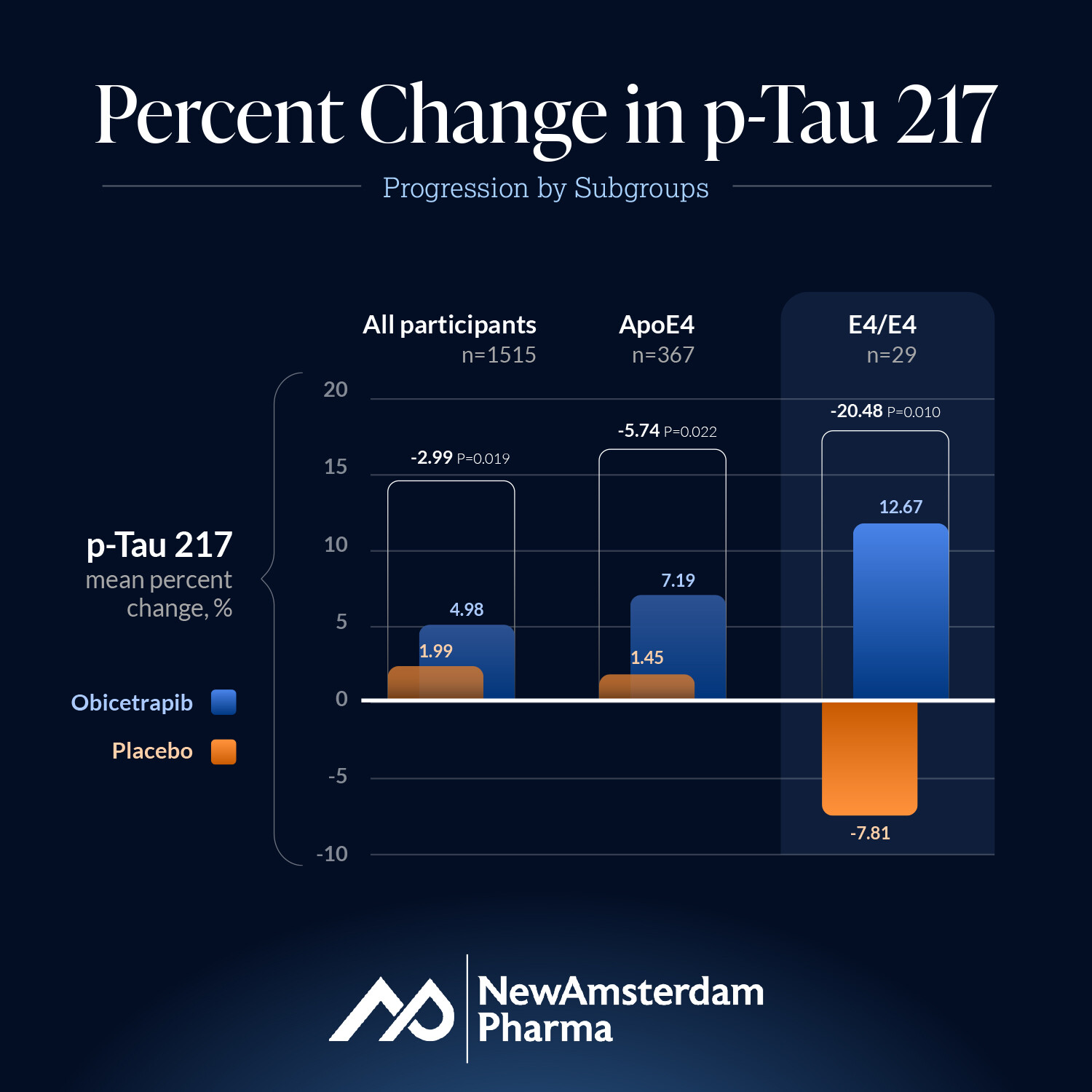
I think they screwed up the legend in the version you posted. What interests me here is that, on placebo, there is a clear pattern where one e4 makes p-Tau 217 accumulate faster than no e4, and homozygous e4 accumulates even faster. What’s interesting is that the impact of Obi is strong enough to regress p-Tau 217 accumulation in homozygous e4 but only slows accumulation in the others.
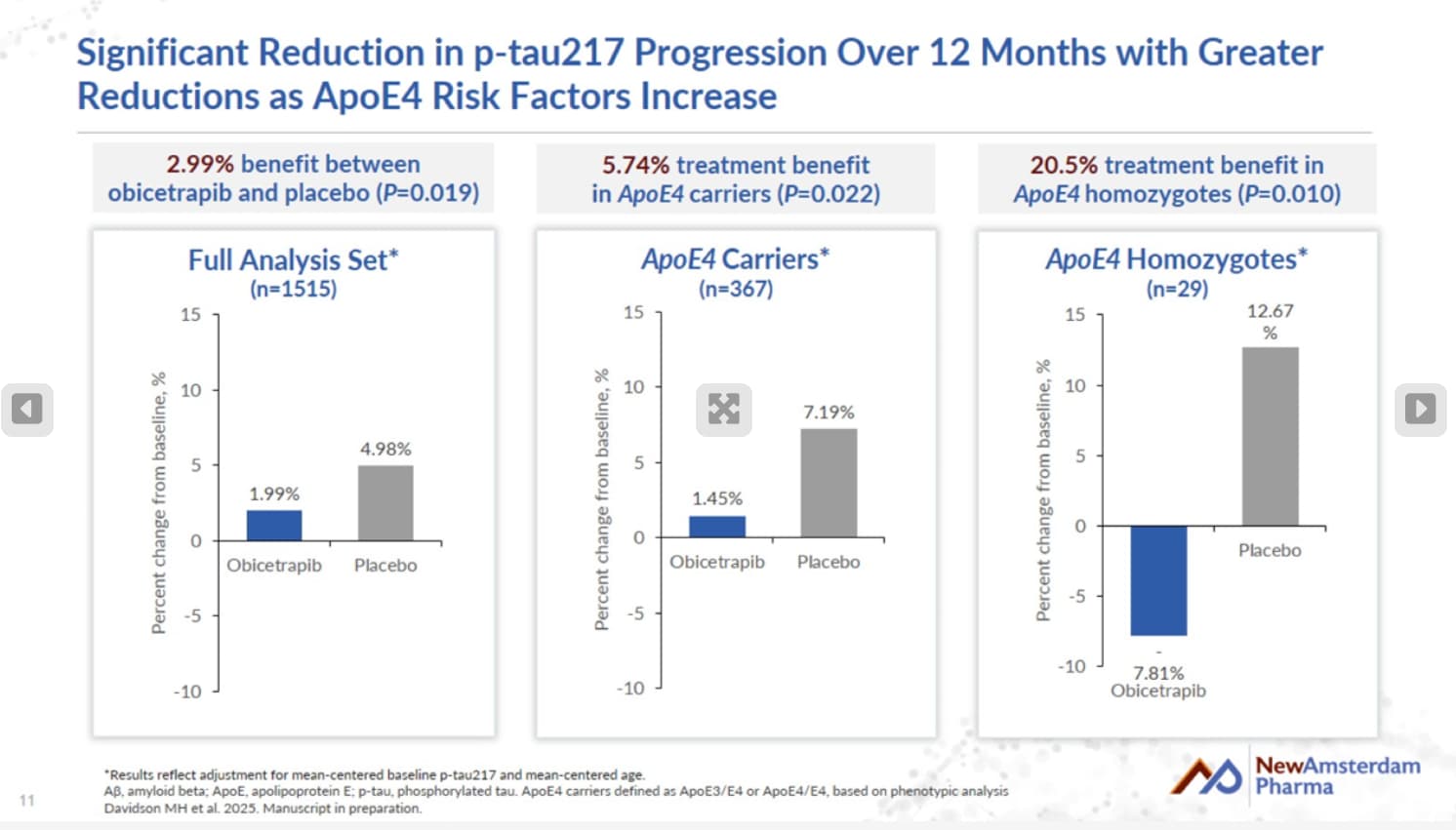
The ‘All prticipants’ graph shows that those on obi saw a 1.99% increase in p-Tau217 levels, whereas the placebo group saw a 4.98% increase. Hence a 2.99% reduction for obi vs. placebo
The ApoE4 subset saw a 1.45% increase on obi vs. 7.19% increase for E4’s on placebo. Hence 5.74% reduction.
E4/E4 saw a 7.81% DECREASE vs. 12.67% increase for E4/E4’s on placebo. Hence 20.48% reduction.
https://ir.newamsterdampharma.com/events/event-details/newamsterdam-conference-call-aaic-2025
4 Likes
Ergo the legend was reversed as suspected. Interesting that E4/E4 is worst case untreated but best response treated.
Assuming equal randomization to placebo and obi in both the whole study population and the ε4 carriers, that would be roughly 2.16% vs. 4.27% increase in the noncarriers. Not shabby, though it would have been nice to see even a slight a decrease like in the ε4 homozygotes.