zazim
#2054
I agree with that. It’s just that your blind spot is you don’t know what you don’t know.
1 Like
A_User
#2055
I don’t think so, I’ve built my certainty on good evidence.
zazim
#2056
Yes, like I said. A blind spot.
2 Likes
Jonas
#2057
rapamycin or sirolimus can raise cholesterol and triglyceride levels, but it does not seem to increase the risk of heart attack or other CVDs (n=406)
Sirolimus and Cardiovascular Disease Risk in Liver Transplantation
Conclusions
Sirolimus causes hypertriglyceridemia and hypercholesterolemia, but it does not increase the incidence of MI or other CVDs. Considering the SRL Cohort has more cardiac risk factors and nearly double 10-year predicted CVD risk, the fact that the CVD incidence is similar suggests that sirolimus is in fact cardioprotective.
https://journals.lww.com/transplantjournal/fulltext/2013/01150/Sirolimus_and_Cardiovascular_Disease_Risk_in_Liver.31.aspx
2 Likes
LDL goes up inflammation goes down. Colchicin evidently works by keeping inflammation in check. Personally I see no reason not to take both rapamycin and a statin.
2 Likes
That is good news, and thanks for posting. I’m not sure I want to bet my life on a single study like this, but lets keep an eye on these types of studies. It would be more compelling if it was a study done in healthy populations, but I doubt we’ll ever that that.
3 Likes
Bicep
#2060
To be fair, it could also be that the Framingham heart model is flawed.
LaraPo
#2061
So did I after developing some palpitations. Continue with Glycine only.
2 Likes
scta123
#2062
But limited knowledge and experience.
zazim
#2063
31% of the people receiving Sirolimus also were on a statin versus 8% in the control group. I wouldn’t bet my health on this study either.
5 Likes
After about 1 year on Rapamycin, I have had an arterial carotid scan and no plaque was noted. Also had a check for Afib and blood circulation. Everything is within normal parameters so it appears that Rapamycin did not affect any of these things detrimentally.
4 Likes
LaraPo
#2065
I also had arterial carotid scan after a few years on R and no plaque accumulation was found.
2 Likes
zazim
#2066
This is an interesting study of a middle-aged, asymptomatic cohort. It shows the limits of a CAC or CT angiogram. [I say this as I go in for one Monday morning.]
60% had subclinical atherosclerosis and nearly half the participants presenting with intermediate or generalized disease. But only 18% had a positive CAC score (with only 4% above 100). Unfortunately, even a CT angiogram would not have detected the soft plaque in the arterial walls that isn’t yet in the lumen of the arteries (quote from another cardiologist talking about this study).
https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.114.014310?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed
“The prevalence of subclinical atherosclerosis (presence of plaque or CACS ≥1) was 63%. Plaques were detected by ultrasound in 60% of participants (31% in the carotids, 25% in the aorta, and 44% in the iliofemoral arteries), and 18% had CAC (CACS: 1–99 in 14%, 100–399 in 3%, and ≥400 in 0.7%). In men, subclinical atherosclerosis was more prevalent (71% versus 48% in women) across all vascular territories, with differences most pronounced in the iliofemoral and coronary arteries (Figure 1).”
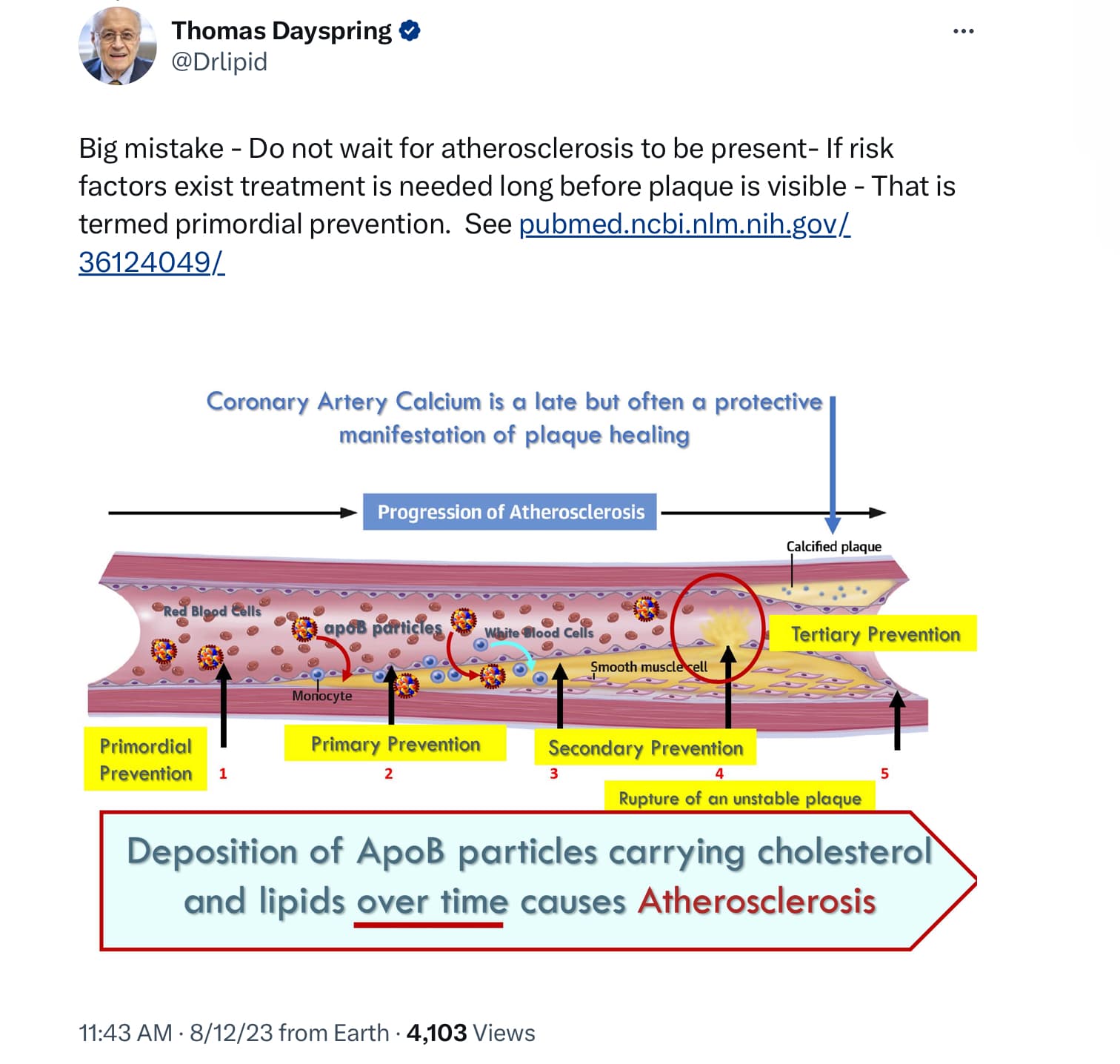
Separate tweet by Dayspring (not referencing this study).
9 Likes
That’s a very interesting study and one that I never saw. It was very informative.
My initial interpretation is that a young person may have a high incidence of subclinical atherosclerosis , even with a CAC of zero, and the most likely area is the ileofemoral.
So in this group it would seem wise to get a 3 d ultrasound of other vascular areas, especially the ileofemoral. It could also be argued that you just skip the CAC in this group and go right to the ultrasound. Of course, since this group was asymptomatic and many considered low risk, how practical is it to test everyone, even though it would be best to do so?
In someone say 65 or older with a CAC of zero, and therefore a very good 10 year or greater prognosis in terms of a cardiac event, perhaps additional scanning isn’t necessary, since it most certainly takes a long while for the subclinical disease to manifest as an event. However, even here, the exception would be if you intend to live to be 100 ( or more), in which case the ileofemoral ultrasound would be helpful.
What are your thoughts?
4 Likes
zazim
#2068
My take away from this is that it is beneficial to aggressively reduce ApoB if it is elevated rather than waiting for damage to manifest itself. That is certainly what I am going to do.
2 Likes
scta123
#2069
That what was done on my last ASCVD risk assessment. My friend and cardiologist said that in my age (48) and being a low risk patient there is no need to do CAC as it will probably be 0 and would not give any additional info and would be just an unnecessary procedure.
2 Likes
i mean more on a societal scale. If half of females and 70% of males have some degree of atherosclerosis in their 30"s , do we evaluate everyone somehow? Is that in any way practical? Do we put them all on meds for life?
1 Like
A_User
#2071
This has also been shown in autopsy studies of soldiers dying in war but I forgot about that. Percent of servicemen with atherosclerosis has declined from the Korean War, to Vietnam War, to recent wars. Yes until there is apoB-lowering vaccines or gene therapy IMO. PCSK9 inhibitors can cost $180/month without insurance (Pravulent, 150 mg x 1 month).
It was pretty self-evident in the first place that atherosclerosis was developing because of CAC being positive for 95%+ of people above age of 70. It is of course a gradual process.
1 Like
José
#2072
FWIW
If I recall;
The doctor who first reported this,{autopsy studies of soldiers dying in war
was Caldwell B. Esselstyn, Jr., MD
1 Like
So the question is, what percentage of the high number of people with atherosclerosis will go on to have an actual clinical event?Do many of them have very slow progression or develop plaque stabilization? Do we screen everyone at a young age? And then what?
1 Like