I totally understand the desire to eliminate every single hint of a risk factor. Too bad that the medical interventions come with side effects.
1 Like
MAC
#771
Here’s a 2 year RCT study on rapamycin with mention of lipids:
Two-Year Randomized Controlled Prospective Trial Converting Treatment of Stable Renal Transplant Recipients With Cutaneous Invasive Squamous Cell Carcinomas to Sirolimus
https://sci-hub.se/10.1200/JCO.2012.45.6376
“The target blood level of sirolimus was 5 to 10 ng/mL, daily dosing”
“Other laboratory investigations (cholesterol, HDL cholesterol, LDL cholesterol, triglycerides, glucose, hemoglobin A1c, albumen, hemoglobin, leukocytes, and platelets) remained stable between start and end of the study.”
No mention of statins or other CVD risk interventions.
4 Likes
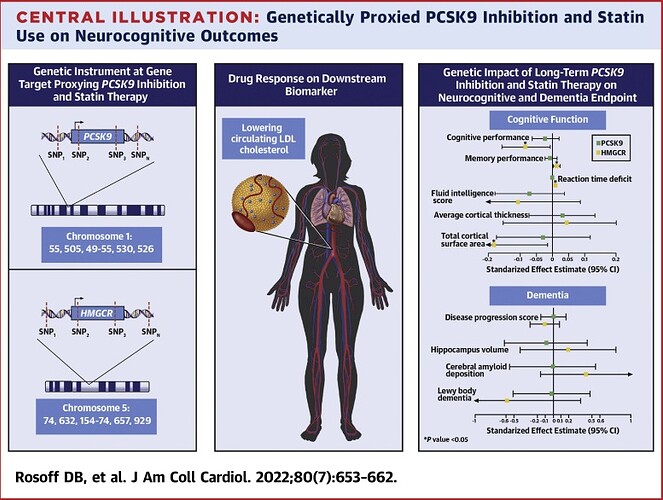
Once again we must recognize that medications aren’t risk free . When deciding on a statin for rapamycin induced lipid elevations, here’s a MR study of 740,000 participants looking at statins and cognitive function.
Statins reduce cognitive function, reaction times, and brain cortical areas.
2 Likes
Davin8r
#773
Glad to see no adverse effect of PCSK9 inhibition. I really like ezetimibe, btw. Not nearly as potent as a statin, but perhaps enough to safely and cheaply reverse the “rapa bump” in lipids? I’d also hypothesize a long term cognitive benefit from the fact that ezetimibe cuts absorption of dietary oxidized cholesterol by 50%, last I checked.
Of course, as we’ve both mentioned, there’s also a very good effect from Amla and citrus bergamot, comparable to meds but safer.
1 Like
MAC
#775
This is interesting, lots of theories as to mechanisms for statins and cognitive, especially since statins work at the liver, and the brain makes it’s own cholesterol. Lipophilicity, metabolities, and BBB could all be in play.
MAC
#776
Indeed. With the literally hundreds of rapamycin studies over the last 20 yrs, you’d think a “cognitive” signal either way would have emerged, but the data is lacking/mixed. Or it could be simply that the cohorts are generally younger, and not yet at cognitive risk steeper part of the curve.
2 Likes
Jay
#777
It’s always a flip of the coin whether I do Cologuard or a colonoscopy. So far I’ve gone with a colonoscopy because of the false positve and false negative rates of Cologuard. I’m more concerned about the false negative rates than the false positives. But, I do give Cologuard serious consideration as that time is approaching again.
https://www.cologuardhcp.com/faq#:~:text=In%20a%20clinical%20study%2C%2013,Cologuard®%20Physician%20Brochure. Page to the bottom to find the following paragraph.
“False positives and false negatives do occur. In a clinical study, 13% of patients without colorectal cancer or advanced adenomas received a positive result (false positive) and 8% of patients with cancer received a negative result (false negative). The clinical validation study was conducted in patients 50 years of age and older. Cologuard performance in patients ages 45 to 49 years was estimated by sub-group analysis of near-age groups.”
Can’t go wrong with either one. Colonguard is easier for sure and is a decent test. Colonoscopy is better if you have a family history or a personal history of polyps.
1 Like
MAC
#779
Re Cologuard…“8% of patients with cancer received a negative result (false negative)”.
“In a clinical study of patients aged 50 to 84 years, Cologuard had an 87% specificity overall, excluding colorectal cancer and advanced adenomas, and including all non advanced adenomas, nonneoplastic findings, and negative results on colonoscopy.”
Overall cologuard has a 13% false negative, when you include pre cancerous.
I’d say you definitely could go wrong with Cologuard and a false negative. That would be way too high for my liking when discussing cancer.
Flipping a coin with cancer? I’d much rather have a trained doctor look under the hood.
2 Likes
Here’s the screening recommendations
Ideally colonoscopy but many people won’t do it. The other options are way better than nothing.
2 Likes
Bicep
#781
I agree with this. Had a neighbor that got terrible infections after and was hospitalized. Mom’s cousin got perforated. The colonoscopy comes with risks too, though if it’s done by a good team I’m sure it’s better than these guys out here in the sticks.
Next time I use the cologuard.
Bicep
#782
I’m not sure where to put this post, but I guess it has most to do with CVD.
Lustgarten talked a lot about oral bacteria becoming the plaque in your arteries. His book is all about microbial burden. In the bloodstream, in the mouth, even on the skin and in the gut. And your ability to fight it becoming worse with age. This has me thinking.
Was it Matt Kaeberlein that talked about oral bacteria or some kind of oral hygiene relative to Rapamycin? Where did I hear that? Is there anything about Rapamycin’s ability to decrease the microbial burden in the gut or in the mouth?
It seems to me that if you are inhibiting TORC1 in your system, then the microbial burden is also exposed to this and I just am wondering what effect it has. Does Rapa kill bacteria in your bloodstream and mouth?
1 Like
There’s this:
I believe Jonathan An is running a study on humans as well.
1 Like
Bicep
#784
Yes, thank you for finding that. And it does support the idea that fixing the microbial burden in the mouth could also fix inflammation in the arteries.
This is probably obvious to you guys, but the large dose every couple weeks probably has a huge effect on the microbial burden overall in the body. Maybe the lipids go up because there is a die off of things in the bloodstream and they have to clean up the mess. Later, the mess is gone and if you keep treating then the burden stays low. The lipids go back down.
2 Likes
Yes, there is a study at the UW Dept of Dentistry on rapamycin & oral health. I think it’s in people, though all I find is about mice.
1 Like
Bicep
#786
I’m a little surprised Rapa has this effect of altering the bacterial load in the oral. It’s not an antibiotic. I don’t understand it, but I still think it is very important after reading Lustgartens book. By what mechanism and in what way does it alter the microbial load?
Also this:
“LDL acts as a carrier for LPS and is involved in mechanisms to inactivate it. Collectively, these data provide further support for the hypothesis that aging and the progression of CVD are associated with increased microbial burden.” This is Lustgarten again.
He then shows how a greater load of LPS causes HDL to increase.
LPS is lipopolysaccharide, which I understand to be a chunk of the cell wall of your microbial burden. LPS could also be thought of as “Little Pieces of Shit”. This stuff is bad news and he goes to great lengths to explain it.
So, to take one more swing at it here, your LPS will increase if Rapa kills off a bunch of microbial burden. This will drive up both LDL and HDL, because their job is to clean up the mess. As time goes on the mess will be cleaned up, the microbial burden will stay low and your lipids should decrease to normal. I think this explains it, but my problem is that nobody is really talking about it and Rapa is not a big killer of bacteria. Though it’s presence may push on the scale in favor of the friendlier bacteria. Why is nobody looking at this?
3 Likes
It’s all very interesting. Here’s a look at the role of cholesterol and its sub components in fighting and preventing infections in layman’s terms.
The risk of infections could explain the increased mortality rates seen in large population studies associated with low LDL levels. It’s possible that as a modulator, rapamycin may be setting lipids at an optimal level according to circumstances. This response isn’t fixed but tends to be in flux.
All of this supports my assertions that we basically don’t know what we’re doing when it comes to a very complex system like the human body. This is even true of TC and LDL where it’s very possible to go overboard.
2 Likes
Bicep
#788
Fantastic article and discussion. Most of the research in Lustgarten’s book came from 20 or 30 years ago.
Very complex subject, thanks again.
1 Like
Agetron
#789
NIce! this article makes me feel my current LDL-C of 141 is protective when you take it with a zero CT Coronary Calcium Score. Was as high as 179 in late April of this year. Rapamycin tends to push it up too.
1 Like