Yes, it’s simple.
I started doing them from a sitting position but it quickly got too easy. Even adding weight was easy so I switched to standing.
Both feet on the floor with knees bent just over the toes. Lift the heels to a 30-45 degree angle, that’s the most important part, and repeat.
I do about 60 of them slowly after eating and again in late afternoon and evenings,according to my circadian rhythm.
After about a month of doing them regularly, I’ve lost about 6 lbs. and 1.5 inches or so off my waist. My glucose dropped 5%. I don’t check lipids very often.
6 Likes
Yeah, I’m impressed by this technique and will now recommend it to my patients.
1 Like
More recently HDL to TR ratio seems to be the better indicator of all-cause mortality.
New research / news story:
So, which is most effective? Researchers at the Cleveland Clinic set out to answer this question by comparing statins to supplements in a clinical trial. They tracked the outcomes of 190 adults, ages 40 to 75. Some participants were given a 5 mg daily dose of rosuvastatin, a statin that is sold under the brand name Crestor for 28 days. Others were given supplements, including fish oil, cinnamon, garlic, turmeric, plant sterols or red yeast rice for the same period.
The maker of Crestor, Astra Zeneca sponsored the study, but the researchers worked independently to design the study and run the statistical analysis.
“What we found was that rosuvastatin lowered LDL cholesterol by almost 38% and that was vastly superior to placebo and any of the six supplements studied in the trial,” study author Luke Laffin, M.D. of the Cleveland Clinic’s Heart, Vascular & Thoracic Institute told NPR. He says this level of reduction is enough to lower the risk of heart attacks and strokes. The findings are published in the Journal of the American College of Cardiology.
“Clearly, statins do what they’re intended to do,” the study’s senior author Steve Nissen, M.D., a cardiologist and Chief Academic Officer of the Heart, Vascular & Thoracic Institute at Cleveland Clinic told NPR. By comparison, he says this research shows that supplements are not effective. “They do not promote heart health. They do not improve levels of the bad cholesterol.” Nissen says supplements can be expensive compared to statin medications. Depending on insurance, Nissen says people may pay less than $5.00 a month out-of-pocket for rosuvastatin.
5 Likes
Arhu
#1041
Statins are not intented to lower LDL, they are intented to improve health span and to prevent all cause mortality, this study does not show that statins are superior in lowering all cause mortality vs the supplements at all
2 Likes
Red Yeast Rice contains Lovastatin.
Does anyone know where the actual research paper is published?
Edit: Found It:
Sadly it is a chargeable paper, but it appears they compare 5mg of rosuvastatin to 5mg of the other things. Alternatively it is unclear. 200mg of Red Yeast Rice extract contains 10mg of statin so it is potentially comparing 5mg of rosuvastatin to 0.25mg of the active component of Red Yeast Rice. Alternatively it is unclear and I am not going to pay to find out.
Personally I am not “anti-statin”, but at the same time I am not frightened of things like pterostilbene which are argued to put up LDL-C.
José
#1043
FWIW
You are aware that in the US the manufacturers of ,“Red Yeast Rice” suppliment are required{by FDA] to remove the “Lovastatin” like compound from the commercially sold suppliment.
If you want the entire “Red Yeast Rice” you would have to make/ferment the rice yourself.
Look online there are many videos on how to make/ferment “Red Yeast Rice”
4 Likes
I wasn’t aware of what happens in the USA. I live in the UK. The RYR I buy has Monacolin K in it. It is made in Italy.
If they were testing RYR in the USA without Monacolin K then that is a total waste of time and effort.
1 Like
rivasp12
#1046
This study is an embarrassment. Statins lower cholesterol. No joke Sherlock.
If you’re going to compare to supplements, at least look at Amla and citrus bergamot, two supplements shown to be as efficacious as statins.
3 Likes
Red Yeast Rice without the active component. Well, that’s one supplement I won’t be purchasing again. Wasted money.  Thanks for bringing it to my attention.
Thanks for bringing it to my attention.
- The U.S. Food and Drug Administration (FDA) has determined that red yeast rice products that contain more than trace amounts of monacolin K are unapproved new drugs and cannot be sold legally as dietary supplements.
A supplement with the most important ingredient removed. Utterly ridiculous.
2 Likes
Davin8r
#1048
The FDA is not enforcing the removal of monocolins/lovastatin from red yeast rice products. Consumerlab.com recently did an analysis of various RYR products, and while the pickings were slim (and multiple brands ARE contaminated with citrinin), Cholestene has been reliable in passing tests for quality (7.5mg lovastatin per capsule) and purity (0mg citrinin) and is the only brand I’d use.
I’m certainly not anti-statin (they’ve saved thousands of lives in high-risk patients, but I don’t advocate them for our drinking water), but that study is garbage. We know (and the investigators already knew) that none of the natural compounds tested would lower LDL to anywhere near the degree as rosuvastatin regardless of dose (except high doses of Cholestene/RYR). The supplements are mainly meant as anti-inflammatory compounds, and many also have platelet-inhibitory (i.e. “blood thinning”) effects and also don’t have the same potential side effects of statins. They are not LDL-targeting agents, with exception of RYR. The experimenters clearly had an agenda.
4 Likes
Can I ask what your LDL-C, or LDL-P, or ApoB is? Do you know?
People with Familial Hypercholestoremia (genetically high LDL-C and ApoB) have heart issues and death earlier in life and more frequently.
How does that square with the notion that “the higher the TC, & LDL, the longer people live” ?
On the internet anyone can find a study or expert supporting every position possible position.
4 Likes
Davin8r
#1050
I know this is a long thread, but we had some good debates and this has been discussed/debated ad nauseum. The hardcore anti-cholesterol folks try to use epidemiological data to support their argument that there’s no causal link (or even an inverse link) between LDL and mortality, when by definition correlational data does not establish causality. Some also use straw man debate tactics such as “if LDL were THE CAUSE of heart disease, then statin drugs should completely eliminate heart disease, and since they don’t, LDL doesn’t cause heart disease”. There’s an abundance of experimental evidence and Mendelian randomization studies which conclusively demonstrate causality.
Dr. Rivasp12 has made some great points along the way, mainly in my mind that establishing background risk is key to how aggressively one might pursue lowering lipids and that absolute risk reduction is often quite small and completely ignored in favor of more impressive-sounding relative risk reduction in drug trials. I think we’ve both emphasized the fact that there are other causal factors involved in CVD, especially inflammation.
I’d really like to see a review paper on comparative absolute risk reduction for CVD outcomes between modifiable factors such as exercise, diet and statins for heart disease, both for primary and secondary prevention. Does having a high VO2 max, for instance, dwarf the effect of any risk reduction you’d ever get from diet or meds?
8 Likes
Don’t the Mendelian randomization studies show that if you take out lifestyle factors, ApoB is a cause of heart disease? I don’t anyone disputes that ApoB in an unhealthy environment can increase risk.
I totally agree. There’s no doubt about the value of statins in secondary prevention as well as the high risk patient.
I too would like to see some studies looking at primary prevention and comparing things like VO2 max, omega3’s index, inflammatory markers, and even Amla and citrus bergamot with statins. Look at absolute risk reduction of total mortality rates.
With primary prevention, and this includes most people on rapamycin I assume, it’s all grey and hazy. Which lipid particles matter the most, oxidized or not, small or large in size, non HDL or APoB, the role of triglycerides and HDL?
How exactly are statins working? Is it lipid lowering, anti inflammatory, both, or something else? Is the benefit/ risk worth the side effects for the otherwise low risk person?
Is rapamycin protective to the point that the lipid elevation is irrelevant? Is the lipid dysregulation just transient anyway?
No one has the definitive answers. I don’t care who they are.
3 Likes
Davin8r
#1053
Oh I agree it’s well established that ApoB-containing lipoproteins are a big underlying causal factor. I was just emphasizing that multiple causal factors converge to give us the end result of unstable atherosclerotic plaques.
2 Likes
I may be wrong here, but from what I understand, from the mendelion randomization studies and what I have heard from Dr. Tom Dayspring, ApoB particles can pass through and get stuck in the endothelium in perfectly healthy individuals. Meaning, high enough concentrations of ApoB is sufficient, in itself, to cause CVD.
2 Likes
Davin8r
#1055
I see ApoB-containing lipoproteins as necessary but not sufficient. After all, we all have AboB particles, yet only some of us have significant arterial plaques. There are other, highly significant factors at play.
2 Likes
A_User
#1056
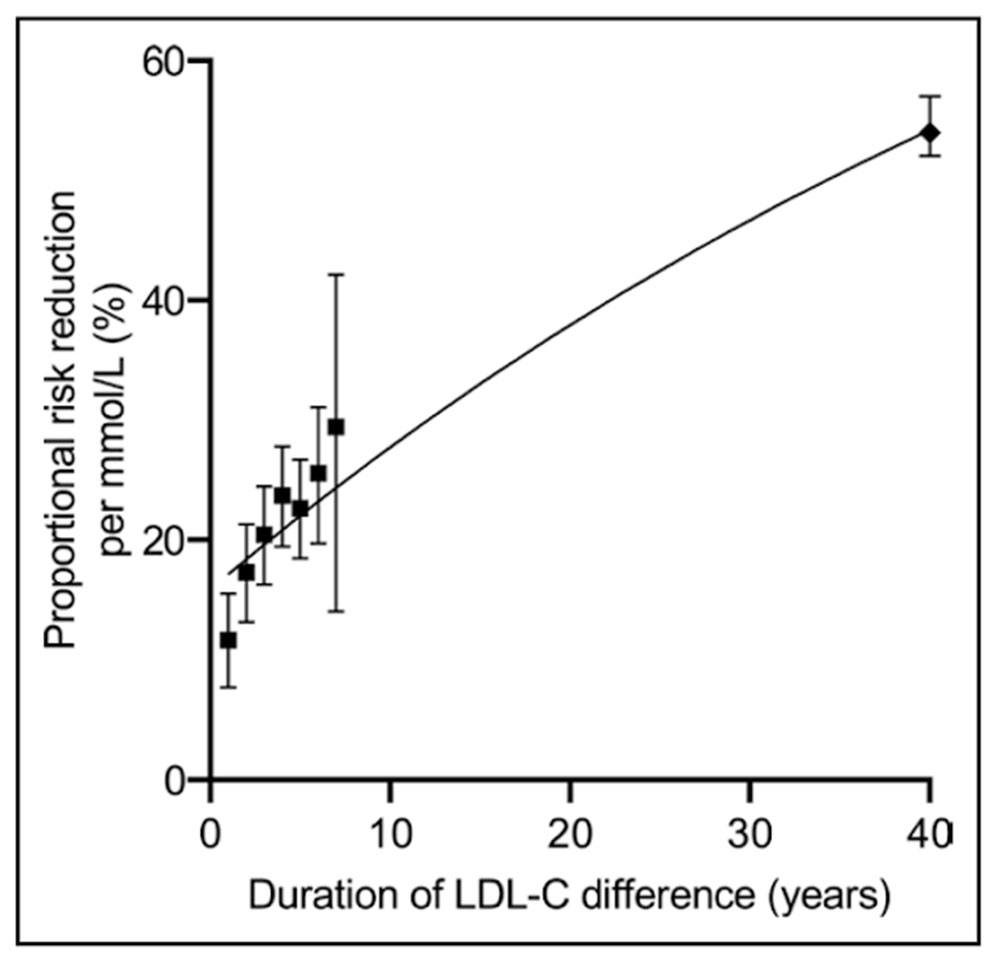
The mendelian randomization results show that the duration of the LDL lowering matters, people are put on statins after 20 or 30 years or longer of damage from above optimal apoB concentration.
It is the apoB amount that matters and duration.
If there are other significant factors there wouldn’t be a such a positive mendelian randomization result.
See the compounding effects of per mmol/L reduction in LDL-c, the last point is from mendelian randomization. And LDL-c is a good proxy for apoB.
4 Likes




