L_H
#1869
Hi apoB and non-hdl cholesterol do correlate. But if you eat a lot of fish the correlation is less strong. (Fish oil changes/improves the particle size and so more cholesterol volume can be transported with fewer apo-b. Its apo-b which better correlates with cvd risk.
So you may be in much better position than your cholesterol results would suggest. Apob really is the gold standard test now. L
3 Likes
zazim
#1870
Unfortunately, I didn’t get any other blood work done apart from testing for omega-3’s. I had gone in to get tested for the ageless rapamycin program. They couldn’t find that paperwork. I had paid for these tests last year and never completed them.
1 Like
zazim
#1873
As best I can tell this is a very inexpensive drug if it is covered by insurance. But close to $400 if not. It does seem very promising.
1 Like
SUMMARY: Niacin should not be used as it lowers lifespan and does not protect against cardio death. It seems to raise blood sugar as well and has other side effects.
My interpretation is niacin magnifies the negatives of Rapamycin further negatively affecting lifespan. If you take Rapamycin, statins are a better alternative for lowering LDL. Do not use niacin with Rapamycin.
Dr. Stanfield weighs in on statins and niacin for cardiovascular protection.
6 Likes
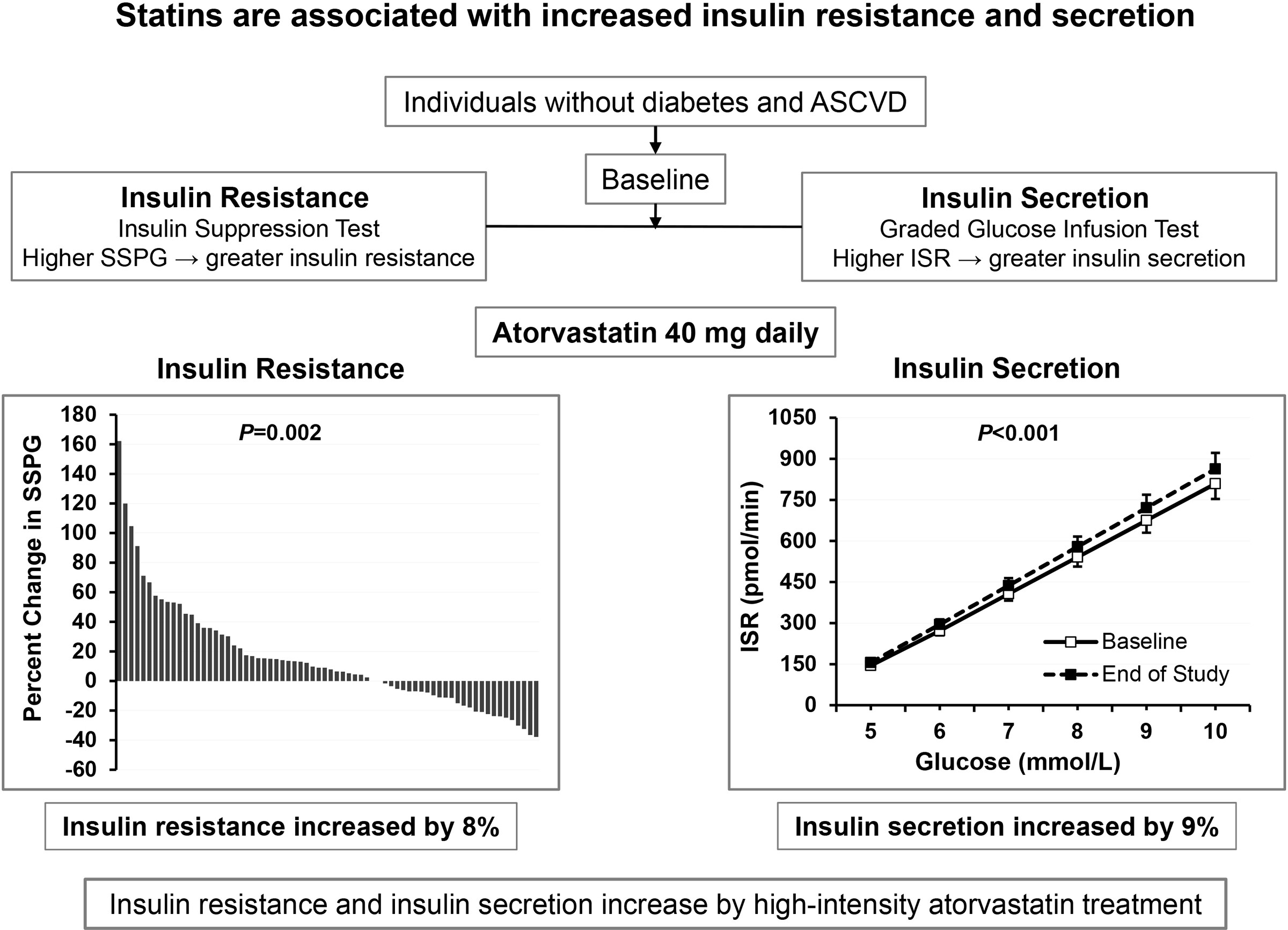
I was skimming through Alan Green’s website and it looks like he recently added a comment about statins. He says that some of his patients have been attempting to significantly lower their lipids with statins ,and these patients are developing significant insulin resistance as measured by HOMA-IR.
I’m not at all familiar with this.
3 Likes
scta123
#1876
Another reason why I am cautious using statins as primary prevention strategy in ASCVD and people advocating it.
2 Likes
Whether or not you want to use statins is of course your choice. But if you think high LDL is okay you are on the wrong side of the science.
Cardiovascular disease is far more likely to kill you than a “modest” increase in insulin resistance
“Statin treatment reduces the risk of atherosclerotic cardiovascular disease but is associated with a modest increased risk of type 2 diabetes, especially in those with insulin resistance or prediabetes.”
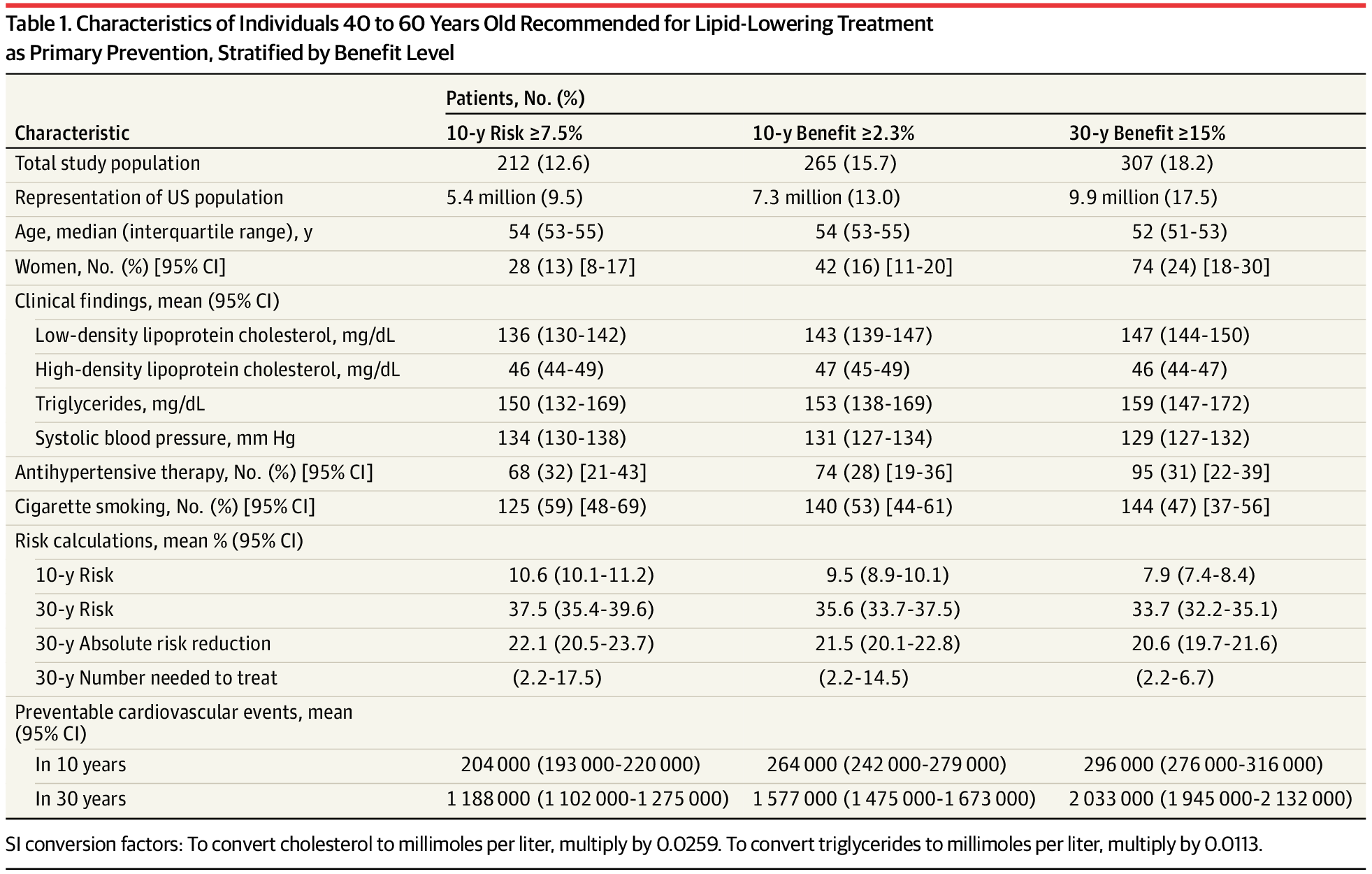
“Given the evidence in favor of statins, as well as the highly
favorable cost-effectiveness profile demonstrated by others at
low risk thresholds (ie, <7.5% 10-year risk), it has been proposed
that statins could be recommended in very broad segments of
the population (eg, to treat all individuals aged 40-75 years).”
“A Long-term Benefit Approach vs Standard Risk-Based
Approaches for Statin Eligibility in Primary Prevention”
https://www.ahajournals.org/doi/full/10.1161/ATVBAHA.121.316159
6 Likes
A_User
#1878
Nothing you can’t measure and fix by stopping statins, changing to something else. I don’t think everyone gets that side effect.
A_User
#1879
Dr. Gil Carvalho delivering the Coup de grâce to the low LDL association debate:
People who advocate atherogenic lipoprotein levels because of low LDL assosciation studies should be ready to become obese, have hyperglycemia and high blood pressure. Cuz they are assosciated with lower mortality. “U-shape” curves.
3 Likes
That was actually very good. Thanks for that.
Of course, even in the conditions he mentions, we wouldn’t want a blood sugar under 60, systolic BP under 90, or BMI under 18. So there is a lower limit.
I’m becoming persuaded that ApoB/ApoA-1 ratio is a good prognostic indicator with under 0.8 being ideal.
Still not convinced that statins are worth the side effects in the low risk patient where the absolute risk reduction in total mortality is less than 1%.
The dose of statin required to get to very low ApoB levels is often quite high and I’m still concerned about the long term impact on cognition and insulin resistance at high statin doses particularly.
I think that bergamot and amla are good alternatives. In the high risk patient, PCSK-9 inhibitors have come way down in price and offer a very good alternative.
Can you get Too low with LDL ? Maybe not, but I believe that the jury is still out with that one.
3 Likes
He properly explains the fallacy of many U-shaped curves.
“Can you get Too low with LDL ?”
As far as I am concerned the point is moot. I don’t think too many rapamycin users are in any danger of getting their LDL too low, quite the opposite in fact.
3 Likes
José
#1883
FWIW
In my view, one of the many compound what I would use/try before any statin.
1 Like
jjrap1
#1884
“I think that bergamot and amla are good alternatives.”
What do folks believe are reasonable doses of these as statin alternatives? 1g qd of each, or ??? Currently taking rosuvastatin but I would like to do an n=1 experiment, try these for a couple months, then get my LDL re-tested to see the effect.
scta123
#1885
Even Thomas Dayspring would agree here.
1 Like
Please, please, explain why statins are so scary for you. Millions of people have benefited from them. All of the alternatives are basically sh*t when compared to the effectiveness of statins and are only used for the small percentage of people who cannot take statins because of the side effects. And the alternatives are not necessarily without adverse side effects.
You doing a disservice by scaring people off of statins that really need to take them.
I am not advocating statins for low-risk people or anyone. But, I would certainly listen to my doctor with an MD over practitioners of alternative medicine.
3 Likes
Seems pretty reasonable.
Your prior posted articles persuaded me to look into the ApoB/ ApoA 1 ratio more carefully, and it’s fairly compelling.
2 Likes
So the studies have mainly been on 1000-1500 mg of CB and 500 mg of Amla.
1 Like
A_User
#1889
You haven’t said what your apoB level is yet rivasp, amla supplements/citrus bergamot isn’t interesting to to many of us unless people start reporting their results.