In my opinion (from a non-doctor) it would definitely be prudent to stop taking rapamycin a few weeks prior to any surgery. You want to get it out of your system so that there is no risk of delayed wound healing.
Here is some research below that I found when searching on “surgery and sirolimus”. This research is focused on transplant patients (who have to take rapamycin - so the bias is to balance the risk of organ rejection vs. recovery from surgery) but it nevertheless seems to have some good points. Since you have no risk of organ rejection (I’m assuming), you can be more conservative and get off rapamycin earlier, and restart it once you are fully healed.
But of course - discuss this with your doctor before you make any decisions.
Minor surgery
Simple uncomplicated wound-closures for skin and subcutaneous surgery, and surgery performed laparoscopically, are unlikely to be affected by the impaired wound-healing induced by sirolimus. It is recommended, therefore, that in this setting any current sirolimus treatment remains unchanged. However, if the patient has one or more of the risk factors identified for impaired wound-healing (Table 1), the advice would be to proceed with caution, and to consider lowering the dose in these particular patients. This approach is also recommended for hernia surgery, where healing of multiple tissue planes is required for successful repair.
Major surgery
The relatively long half-life of sirolimus necessitates that the drug is discontinued 5–10 days before planned major surgery in order to avoid any postsurgery complications such as impaired wound-healing, as described previously.
Steroid adjustment around surgery should follow standard published guidance in this area [39], or local protocols. If the patient is receiving a combination of sirolimus and mycophenolate without steroids, low dose steroid should be introduced following sirolimus discontinuation.
After surgery, we would recommend re-starting sirolimus treatment after 1–3 months, or when any courses of chemotherapy have finished.
Any deterioration in renal function should be promptly investigated and renal biopsies may be required to exclude an acute rejection episode in this setting. If there were to be a rejection episode in this setting, then treatment depending on the primary surgical problem will require to be carefully customized.
Emergency surgery
In the event of emergency surgery, sirolimus should be stopped as early as possible, again to limit any possible impaired wound-healing responses. As with major surgery, the use of steroids as immunosuppressants is recommended (Fig. 2). With respect to these recommendations, it may be noted that sirolimus could be re-started 5 days postsurgery: this should be sufficient time to avoid an impaired wound-healing response. In the case of emergent surgery necessitated by cancer, the line of recommendation set out for general major surgery from the point of differentiating cancer-related and cancer-unrelated surgery can be followed, although it should be borne in mind that such circumstances will necessitate case-by-case considerations.
Source:
In another paper… again, for transplant patients - so already you have a group of people taking many medications (frequently) and who may be quite sick:
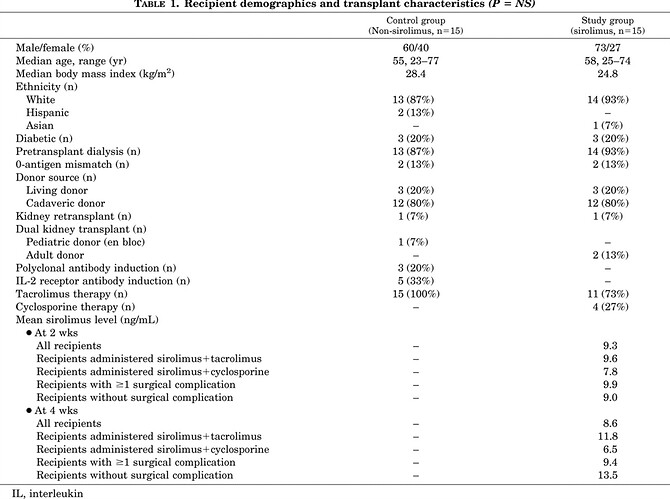
When we began to use sirolimus for induction after KTx, we observed not only more frequent lymphoceles but also a higher rate of other surgical wound complications. Unfortunately, clinical sirolimus studies have mainly focused on immunologic efficacy and nonsurgical complications (1). In a case-control study, we compared surgical wound complications in recipients treated with and without sirolimus.