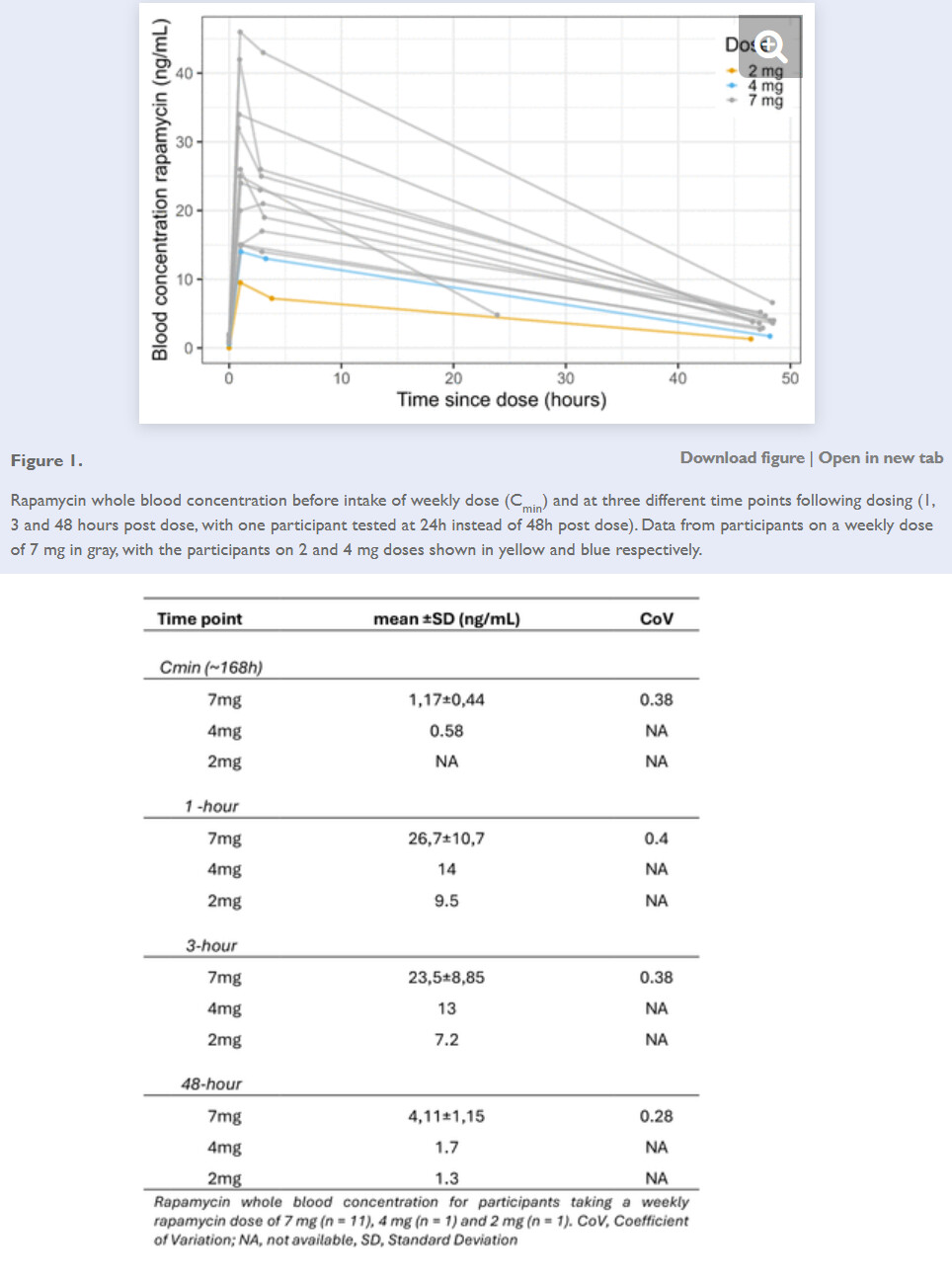
Any thoughts on Yuri’s X post: “More evidence that people taking weekly rapamycin could be putting themselves into immunosuppression for days at a time. Here’s a rapa PK study showing that people taking 7 mg per week have their blood levels at 4 ng/mL two days after dosing. Moreover, even 7 days after dosing, their blood levels are at 1 ng/mL. Target immunosuppressive blood levels are 5-15 ng/mL. As many rapamycin biohackers take 10 mg weekly, their blood levels could well be above 5 ng/mL for half the time.”
https://x.com/ydeigin/status/1908569671072100687
Here is the preprint study on people around 60 years old taking rapamycin the brand Rapamune from Pfizer: https://www.medrxiv.org/content/10.1101/2025.03.18.25324017v1.full
PS. My plan is to check my blood levels this in the autumn this year. Just to see how things are for me. Will share it later on with you all.
2 Likes
As I have said previously I think the trough is important as well as the peak. With a half life of 60 hours assumed although this will vary 7mg at the start of a week is equivalent to approximately 1.005111061 mg at the start of the next week.
1 Like
 Have you check your rapamycin blood levels throughout the different dose protocols you have tested and if so what was your findings?
Have you check your rapamycin blood levels throughout the different dose protocols you have tested and if so what was your findings?
I have not done any rapamycin tests. My usual labs dont offer this.
1 Like
KarlT
#5
I would think there would be blood levels well past 1 week based on half life.
1 Like
ORRAPA
#6
So essentially, this is arguing for a daily does instead of a pulsed dose to avoid immunosuppression. I’m going to note the lancet article suggested up to 2mg/day is well tolerated.
1 Like
If one goals a level of 3 ng/mL at 50 hours (weekly dosing) or at 100 hours (q14 days dosing) you’ll have a non-measurable level at time of redosing.
I remain convinced that it is important to monitor as I have individuals who by gender and weight are equivalent, one on 5 mg and the other on 12 mg for weekly dosing, each with blood levels right where we want them.
I know on trough - these individuals, and I had just a few do a level - most commonly accidentally right before taking their dose - and the levels if dosing as I’m specifying are <0.5 ng/mL.
Daily dosing causes immunosuppression as you’ll be sitting at a blood level the entire time that will inhibit mTORC1 and mTORC2 (to some extent).
I’ve have well over 100 patients on Rapamycin, average length of time under my treatment a year right now - but have only had 2 soft tissue infections, both easily treated and also no concerning laboratory findings (e.g. lipids and insulin resistance not significantly impacted).
I’m starting to setup some tables so the data is more readily available, but I usually pick within 1-2 mg of final dose with initial dose - but have had some people’s results be substantially different than anticipated.
11 Likes
Thank you, Dr. Fraser, that’s invaluable real life data you are getting, and pretty unique over a prolonged time frame in the context of non-transplant or immunosuppressive clinical application. Maybe Dr. Green had some data too, but systematic and measured, that’s exceptional. When it comes to rapa dosing protocol, there is no one I trust more than you - you have the data IRL!
1 Like
@ORRAPA I have been thinking more about this and because we have for example low levels of rapamycin in our blood then this does not mean per se that we are immunosuppressant. We can inhibit mTOR without suppressing the immune system. So when thinking more about the topic then I’m not personally concerned about this because I have not seen an increase in either viral or bacterial infection. It’s more the opposite that I have experienced less viral infections then the rest of my family members and working colleagues. So I don’t see that this argues for daily dosing. Joan Mannicks phase one trial showed also that weekly dosing was a little bit better than daily dosing.
@DrFraser Big thanks for sharing your clinical experiences! When I interview in my podcast in the future let’s also discuss this in it  Please keep me updated on how things develop! By the way, what does soft tissue infection mean?
Please keep me updated on how things develop! By the way, what does soft tissue infection mean?
@CronosTempi Here is one thing Dr Green shared about his clinical experience when I interviewed him. Roughly it’s about that the innate system is getting a bit inhibited which increases bacterial infection but the adaptive immune system improves which decreases or mildens viral infections.
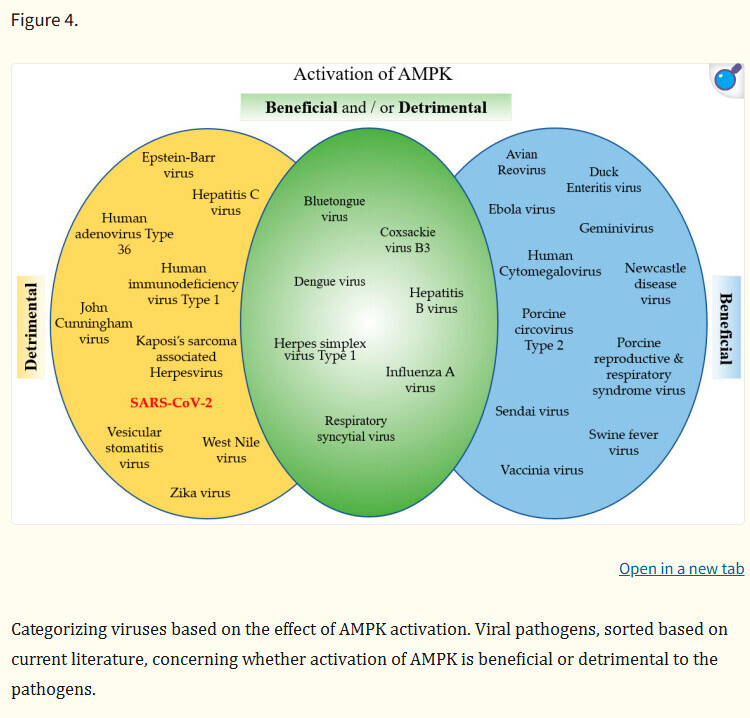
But the immune system is a very complex and activation of catabolic processes like through mTOR inhibition is not always beneficial. I have shared this image before but I think it’s quite interesting image to highlight again which gives a picture of how different viral infections can react to anabolic and catabolic processes.
Source: Multifaceted Role of AMPK in Viral Infections - PubMed
I like this paper contrasting mTOR with AMPK.
The Opposing Actions of Target of Rapamycin and AMP-Activated Protein Kinase in Cell Growth Control
2 Likes
Ah, thanks for sharing that paper by Michael Hall!
Is there a natural equivalent to rapamycin for shutting down the immune system that can be used to assess the human risk to taking rapamycin too frequently or too high a dose such that the trough isn’t zero for long periods of time. Something like long term water fasting or athlete over-training? I understood rapamycin does not shut down anything but just reduces mTORC1 significantly to allow up regulation of AMPK, with the side effect of reducing mTORC2 if mTORC1 is turned down too much for too long. Perhaps this is similar to long term calorie deprivation from very low intake or high exercise energy use with insufficient calorie intake.
For now I make sure I go to zero rapamycin in my blood by using a 14-day cycle followed by a 1-2 week clearance pause every 2 cycles. I also don’t push the dose (roughly 15mg using fat and GFJ with Rapacan). I’ve started combining a monthly FMD with one of my rapa doses.
If anyone can speak with authority on why I’m taking too much or too little I’d like to hear it.
1 Like
Would love to discuss this approach further with you. I’m just starting to put data in a table for all patients I have on Rapamycin.
2 Likes