How to optimize your Levine Phenotypic age, suggestions from CGPT5:
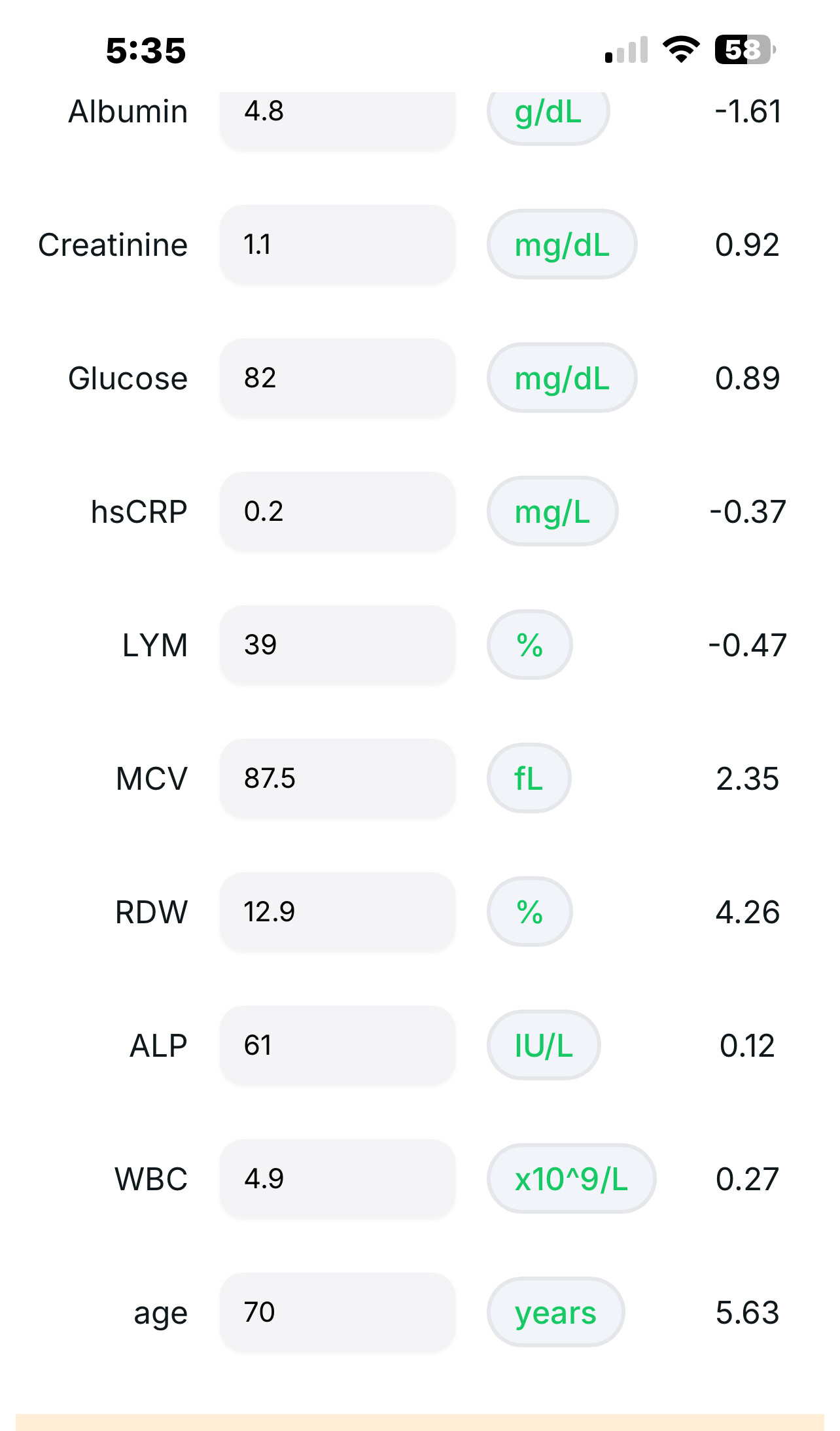
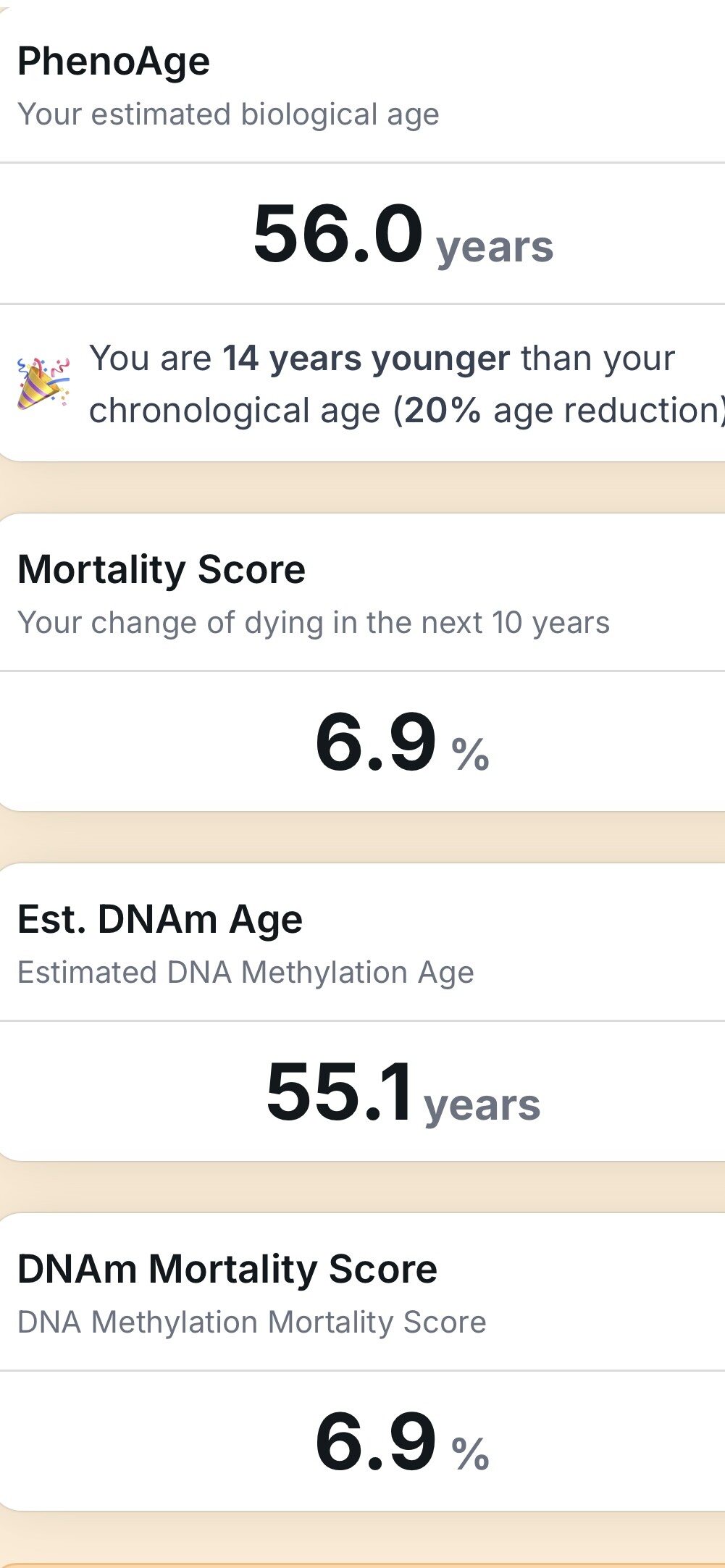
Here’s what’s inside the (Morgan) Levine Phenotypic Age / “PhenoAge” clock, and which direction is “better” for the score:
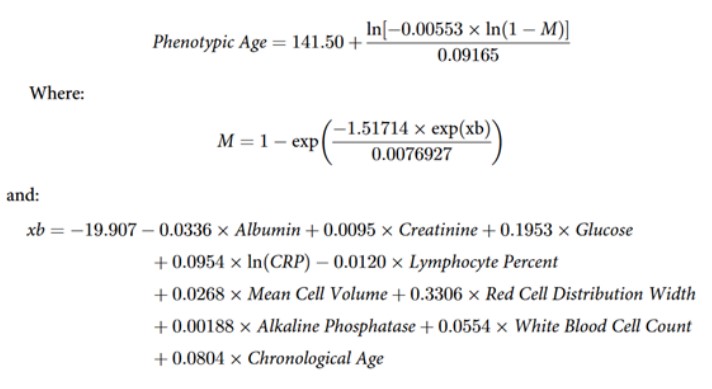
| Biomarker (blood/hematology) |
“Younger” direction in PhenoAge |
| Albumin |
Higher |
| Creatinine |
Lower |
|
Glucose (fasting) |
Lower |
|
C-reactive protein (hs-CRP; log) |
Lower |
|
% Lymphocytes (differential) |
Higher |
| Mean Corpuscular Volume (MCV) |
Lower (avoid macrocytosis) |
| Red Cell Distribution Width (RDW) |
Lower |
| Alkaline Phosphatase (ALP) |
Lower |
| White Blood Cell count (WBC) |
Lower |
| Chronological age |
included in the model |
Below are practical levers for each marker. These are general, evidence-based ideas—not medical advice. For medications or if your labs are out of range, loop in your clinician.
1) Albumin — aim higher (within normal)
What low suggests: inflammation, liver disease, malnutrition, frailty.
Levers
-
Protein & calories: 1.2–1.6 g/kg/day protein (distributed across meals); add whey/casein if intake is low.
-
Resistance training: 2–3×/wk improves anabolic status and albumin over time in frail adults.
-
Treat drivers: manage chronic inflammation/infection; assess liver function, nephrotic loss, GI malabsorption.
-
Micronutrients: ensure adequate zinc and vitamin D (replete if low).
2) Creatinine — aim lower (protect kidneys)
What high suggests: reduced GFR, dehydration, muscle injury (rarely: very high muscle mass can raise it slightly).
Levers
-
Hydration & BP: keep well-hydrated; target ~120/80 if appropriate.
-
Glycemia: tight glucose control if diabetic; consider SGLT2 inhibitor or ACEi/ARB (clinical decision).
-
Avoid nephrotoxins: minimize NSAIDs, contrast dye; review supplements (e.g., very high creatine can confound).
-
Dietary pattern: plant-predominant, low-sodium; treat metabolic acidosis (bicarbonate) if present (clinician-guided).
3) Fasting Glucose — aim lower (80s–low 90s mg/dL is often a good target)
Levers
-
Diet: minimize refined starch/sugar; 25–40 g fiber/day (psyllium, inulin, veggies, legumes); protein at breakfast.
-
Timing: earlier, consistent meal window; avoid late-night eating.
-
Exercise: post-meal walks or 10–15 min zone-2; 2–3×/wk resistance training.
-
Tools: CGM-guided meal tweaks.
-
Supplements/meds: Psyllium, berberine (300–500 mg 2–3×/day), acarbose, metformin, GLP-1 RA, SGLT2i—discuss with your physician.
4) hs-CRP — aim lower (<1 mg/L ideal)
Levers
-
Weight & activity: 5–10% weight loss and 150–300 min/wk aerobic + 2–3×/wk resistance.
-
Diet: Mediterranean pattern; more EPA/DHA fish; fewer ultra-processed foods.
-
Oral & sleep health: treat periodontitis; 7–9 h sleep; screen for sleep apnea.
-
Stress: mindfulness, CBT-i for insomnia, daylight exposure.
-
Supplements/meds: Omega-3 EPA/DHA 2–4 g/day (TG-lowering doses also reduce CRP); curcumin (bioavailable forms); statins and low-dose colchicine reduce CRP in selected cardiometabolic patients (physician-directed).
5) % Lymphocytes — aim higher (within lab normal)
What low suggests: stress glucocorticoid effect, acute illness, nutrient deficits, autoimmune disease, some meds.
Levers
-
Address causes: review meds (steroids), treat infections, manage autoimmune disease.
-
Sleep & stress: consistent 7–9 h; reduce overtraining; add recovery blocks.
-
Nutrition: replete vitamin D, zinc, selenium, B12/folate if low; adequate protein.
6) MCV — aim lower (avoid macrocytosis >~95–100 fL)
What high suggests: B12/folate deficiency, alcohol use, hypothyroidism, marrow/medication effects (e.g., hydroxyurea).
Levers
-
Test & replete: B12 (consider methylcobalamin) and folate (diet or 400–800 µg/day if deficient); check MMA/homocysteine.
-
Cut alcohol (or keep very moderate).
-
Screen thyroid and treat if hypothyroid.
-
Review meds with your clinician.
7) RDW — aim lower
What high suggests: iron deficiency, B12/folate deficiency, chronic inflammation/CKD.
Levers
-
Find the cause: ferritin, transferrin saturation, B12, folate, CRP.
-
Replete: iron (dietary or oral iron—take with vitamin C, away from calcium), B12, folate as indicated.
-
Treat inflammation/CKD drivers; improve diet quality and activity.
8) Alkaline Phosphatase — aim lower (but not below lab range)
What high suggests: cholestasis/bile duct disease, bone turnover (vitamin D deficiency, Paget’s), certain meds.
Levers
-
Differentiate source: get GGT (hepatobiliary) and ALP isoenzymes or bone markers if needed.
-
Vitamin D repletion to 30–50 ng/mL if low; ensure calcium/magnesium adequacy.
-
Liver health: reduce alcohol; tackle NAFLD (weight loss, exercise, lower fructose/simple sugars).
-
Bone health: resistance & impact training; treat hyperparathyroidism/thyroid disorders if present.
9) WBC — aim lower (but within normal; avoid leukopenia)
What high suggests: infection, smoking, obesity, sleep apnea, systemic inflammation.
Levers
-
Lifestyle: stop smoking/vaping; reduce visceral fat; treat OSA; regular exercise.
-
Oral/gum care and infection control.
-
Anti-inflammatory diet as above; manage chronic conditions (e.g., gout, autoimmunity) with clinician.
Practical playbook
-
Measure right: Use fasting morning labs for glucose and CRP when possible; avoid hard workouts/alcohol the day before.
-
Fix deficiencies first: B12/folate/iron/vitamin D and zinc shifts can improve MCV, RDW, ALP, lymphocyte %.
-
Hit systemic levers: weight reduction, aerobic + resistance training, sleep regularity, oral health, and smoking cessation move CRP, WBC, glucose together.
-
Kidney & liver checks: if creatinine or ALP is off, investigate causes before “supplementing.”
-
Retest cadence: every 8–12 weeks after an intervention block is a reasonable cycle to see movement without chasing noise.