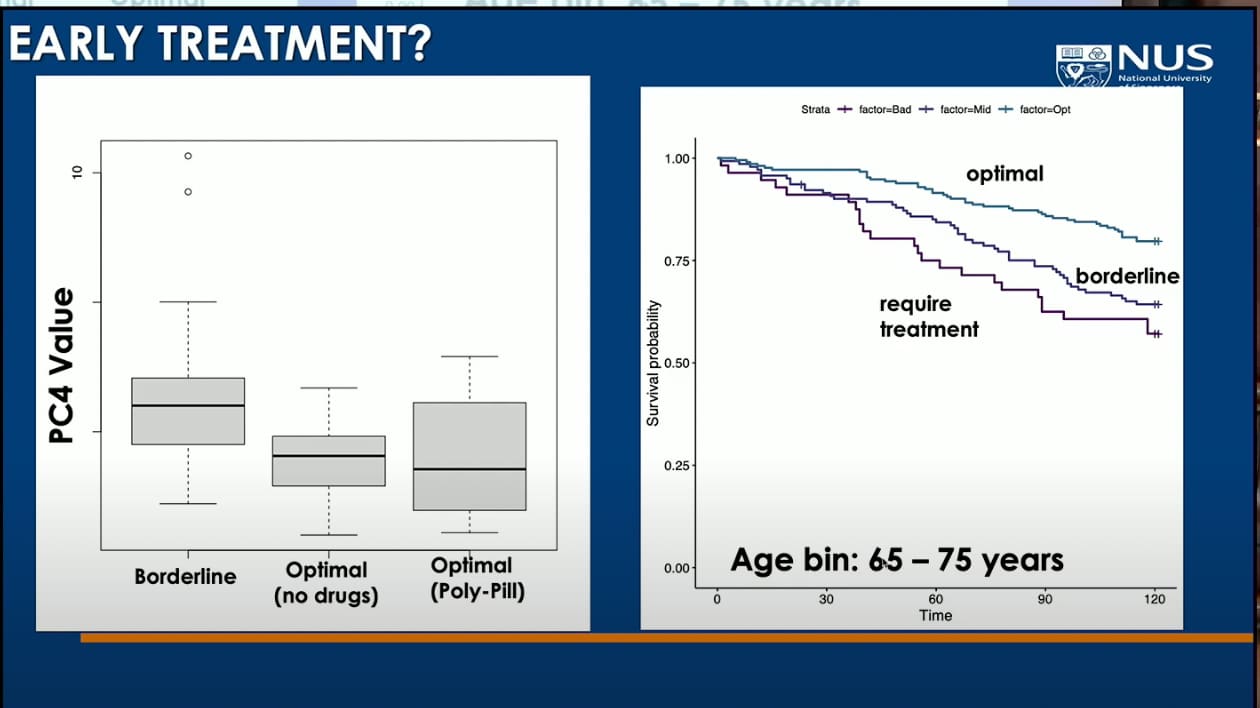
Thank you, RapAdmin, that’s a fabulous video from Brian Kennedy. You picked a great set of graphs from that video showing survival curves for optimal biomarkers, borderline, require treatment, but just a few seconds later the graph becomes even better (~14:30), where we also see the labels, and the treated (polypill) show a beautiful line, the best of 'em.
A couple of casual observations. BK mentions that they’ve had very limited luck combining longevity treatments, because so often those don’t stack, or even cancel each other. Now, those are focused on longevity specifically. But, if we look at treatments that address diseases and therefore prolong life through those means, then the polypill comes out as a kind of star, looking at that graph, pretty robust. And a polypill is a “combination” if there ever was one. Of course one could say that disease treatment is not strictly a longevity intervention, as really in treating disease it merely normalizes lifespan, bringing it back to what it would be without disease, i.e., it abolishes the life-shortening effect of disease. And yes, that is true to an extent, but not entirely, because as the graph shows, treated subjects can exceed the survival of naturally “optimal”, who are of course free friom disease. That shows a small, but significant longevity effect - therefore the polypill qualifies as a true longevity treatment (though clearly rather modest).
This also validates the approach many of us on this site take to medications. We take them, believing that the net effect will be positive. The opposing view - well represented here too - is that it is best to reach optimal biomarkers through lifestyle interventions only, without drugs. It’s what I call the naturalistic fallacy. The superstition, essentially, that somehow “natural” is always superior to the “chemical”, “artificial”, “drugs”, “pharma” and so on. I always saw that as a pernicious idea, because it is the most natural thing in the world to look at results, regardless of how you got there, through “natural” or “unnatural” means. Who cares if you die “naturally” at 85, but live healthily but “unnaturally” to 105. I’ll take the “unnatural” 105 over the “natural” 85 every time. “Unnatural” is the very definition of how civilization is built and progresses. If we only strictly ever adhered to “natural” we’d not only not emerge from the caves, but we wouldn’t even climb down from the trees. Evolve or join the dinosaurs. Science for the win!
Therefore, I for one, have no hesitation about taking pharmaceuticals. So happens, that my lipids are “naturally” trash (despite heroic lifestyle interventions), and so I must take lipid lowering pharma agents. But I’d take statins even if my lipids were “naturally good”, because of the pleiotropic effects anyway - they lower inflammation, which has good health effects. And that way, I get both “good” lipid numbers (as good as “naturally” optimal ones), but in addition might get benefits from the anti-inflammatory or anti-cancer effects. Win-win. Same for my borderline blood sugar. I take empagliflozin, banking that not only will it help my BG biomarker, but perhaps have additional pleiotropic effects (perhaps on kidney health?).
Obviously, what matters here is a careful tailoring of what is in that polypill. Some BP meds are better than others for longevity - and some may even be deleterious. So, in picking my BG, BP, and ApoB polypill, I have to look very carefully at the individual constituents. That’s where the concern of DDI (drug-drug interactions) enters. The dangers of polypharmacy. Yes, it’s something to be concerned with - absolutely. But as this presentation shows, the mere fact of polypharmacy is not deleterious in and of itself - there is room for a sum greater than its parts, because that’s what the polypill result shows us.
Therefore, what we can take away from this is: if you have borderline metabolic biomarkers, it is OK for you to resort to a polypill, as long as you carefully select the constituent ingredients suitable to your unique situation. There is no one size fits all here - some people do better with one drug than another, or have a negative reaction or whatnot. But there is hope - you can go forward with drugs as long as you carefully vet your particular polypill. Or at least that’s what I took from this. YMMV.